


Article Figures & Tables
Figures
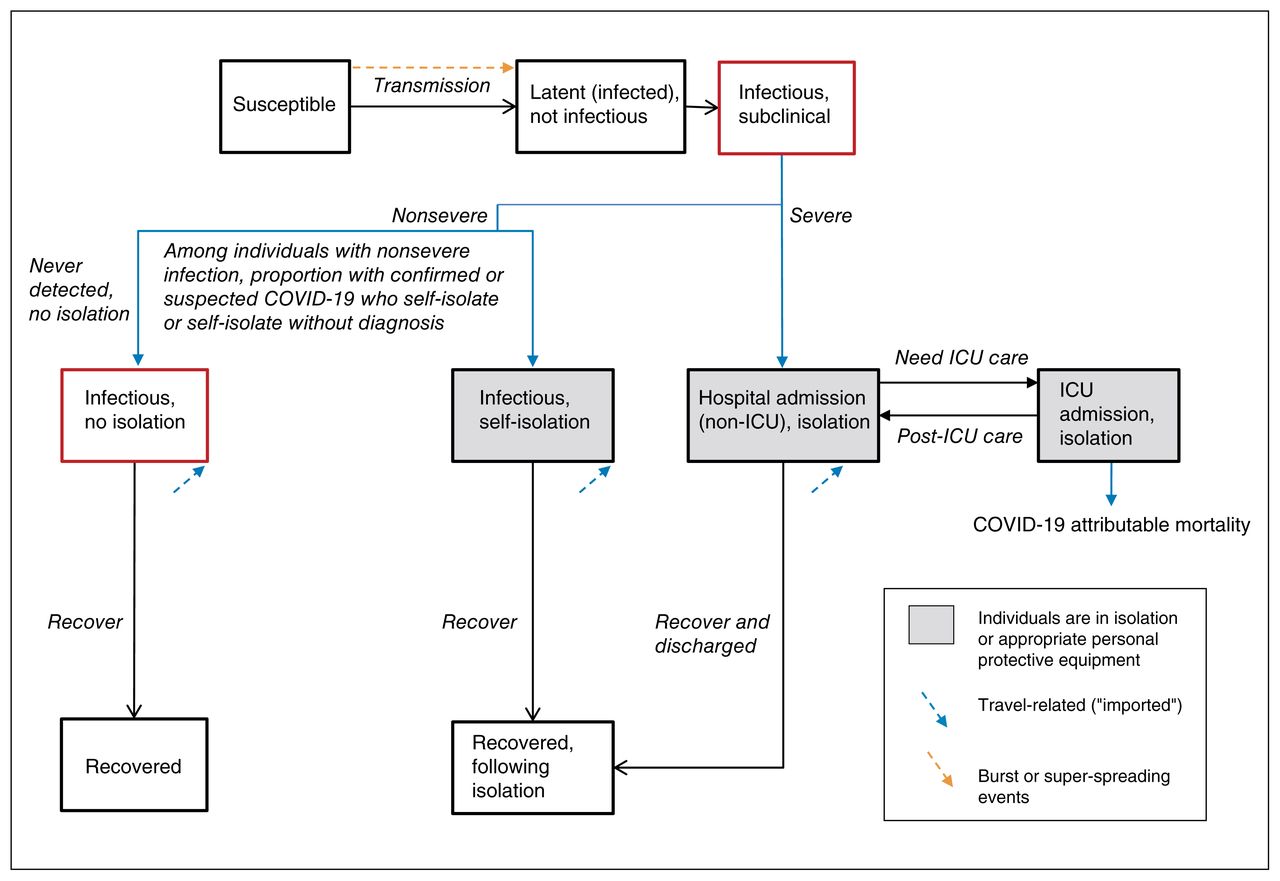
- Figure 1:
Transmission model structure. Compartments represent health states, with transitions between health states in a stable population of fixed size. A proportion of individuals infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) develop severe coronavirus disease 2019 (COVID-19) and require admission to hospital. Among individuals with nonsevere COVID-19, a proportion self-isolate after receiving a diagnosis of confirmed or syndromic COVID-19 or may self-isolate without a diagnosis; the remainder do not self-isolate. Only a subset of individuals with nonsevere COVID-19 receive a confirmed diagnosis if they undergo testing. Individuals in the infectious health states may pass the virus on to others. We assume that individuals in self-isolation or hospital-isolation cannot pass on the virus, but superspreading events are included to capture community, long-term care and nosocomial (hospital-acquired) clusters of transmission events. Note: ICU = intensive care unit.
- Figure 2:
Cumulative detected cases per 100 000 population across simulated epidemic scenarios and observed data used for epidemic constraints. Model outputs from the sampled range of parameters in Table 1, which meet the model constraints are shown for detected cases as solid lines. The observed data for Lombardy, Italy, (61) and Hong Kong, China, (62) are shown as dotted lines, and the corresponding data points at day 30 since the outbreak started were used as upper and lower bounds, respectively, to constrain the epidemics. The observed data on cumulative detected cases for the GTA (travel-related and local transmission) up to Mar. 20, 2020, are also shown (dashed black line) as part of the face validity check. The model output for the fast or large epidemic is shown via the purple solid line and slow or small epidemic via the blue solid line, selected as the upper and lower quartile of peak incidence, respectively, within the first 300 days. The default (solid red line) depicts the default scenario (Table 1). Simulated timeline begins at the start of the “seeding” of the population with 0.0011%–0.0048% of the population already infected with severe acute respiratory syndrome coronavirus 2. For observed data, we defined the outbreak to have started when 3 confirmed cases were observed. We chose 3 cases detected as the onset of the epidemic based on the observed epidemic curve in the GTA, where the curve started to take off after detection of 3 cases (Feb. 23, 2020). We applied the same threshold for other regions for comparability of epidemic curves across geographic locations. Note: GTA = Greater Toronto Area, COVID-19 = coronavirus disease 2019.
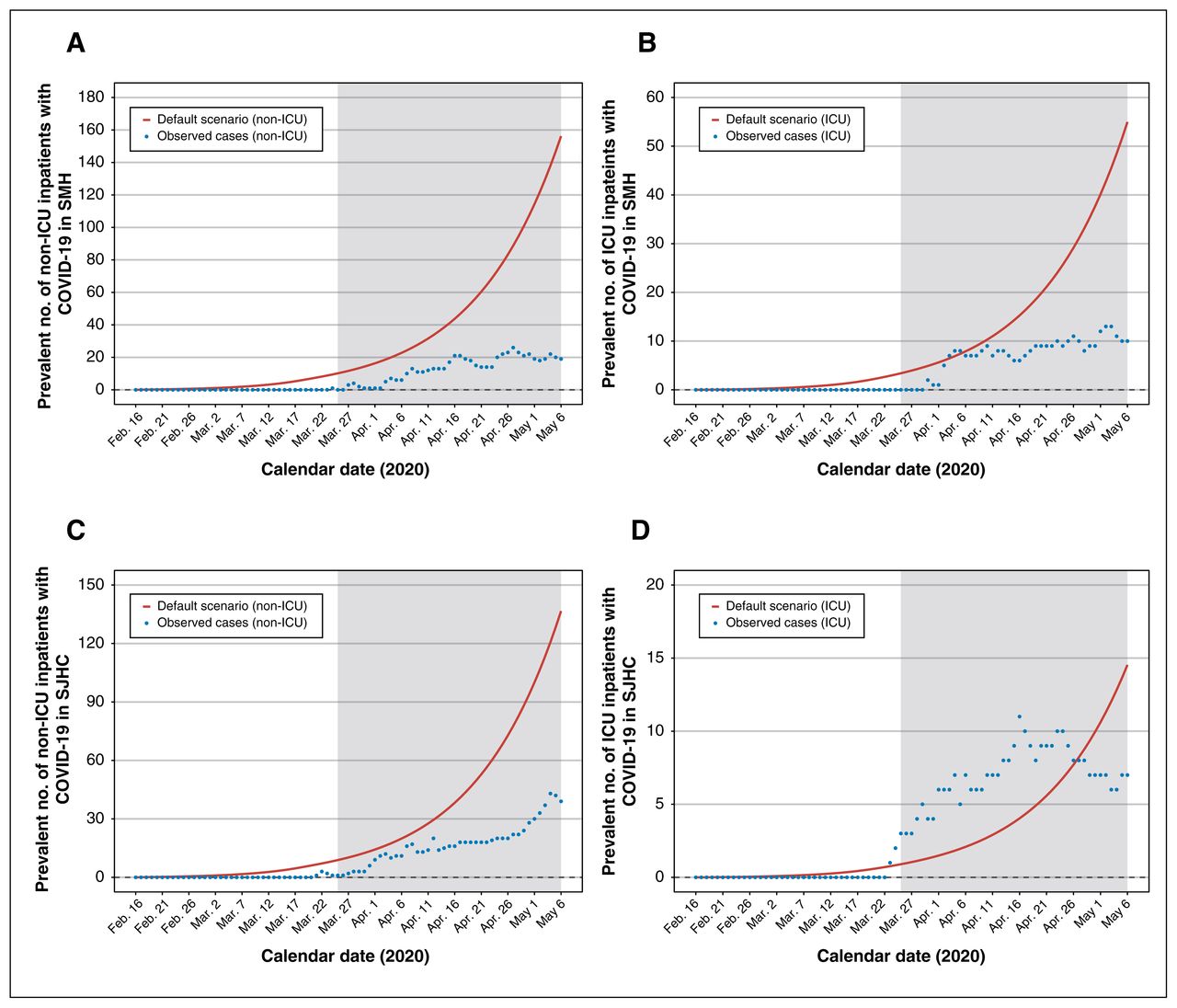
- Figure 3:
Estimated versus actual COVID-19 inpatient census at St. Michael’s Hospital (SMH) and St. Joseph’s Health Centre (SJHC) in the Greater Toronto Area. Model outputs from the default scenario. Observed data reflect the actual inpatient census of laboratory-confirmed cases of COVID-19. Results are shown for SMH (A) non-ICU inpatient census and (B) ICU census; and for SJHC (C) non-ICU inpatient census and (D) ICU census. The shaded area refers to the period of model projections used by each hospital in pandemic preparedness planning. Note: COVID-19 = coronavirus disease 2019, ICU = intensive care unit.
- Figure 4:
Estimated surge and capacity for non-ICU and ICU admissions to hospital at St. Michael’s Hospital (SMH) and St. Joseph’s Health Centre (SJHC) in the Greater Toronto Area. Model outputs from the default scenario under the assumption that pre-outbreak, non-COVID-19 admissions do not change. *Estimated by the median number of non-ICU inpatients at each hospital between March and June, 2014–2019. Observed data reflect the actual inpatient census up to May 6, 2020. Results are shown for SMH (A) non-ICU inpatient census and (B) ICU census; and for SJHC (C) non-ICU inpatient census and (D) ICU census. The dashed red line indicates the inpatient bed capacity. Note: COVID-19 = coronavirus disease 2019, ICU = intensive care unit.




Tables
Variable Units Default value Range examined in sensitivity analyses (uniform distribution) Reference and notes Epidemiological Population size of the GTA Number 6 196 731 NA Projected estimate from 2016 census (7), (8) and a 1% annual change as per the United Nations Urbanization Prospects, (9) and using the census metropolitan area of Toronto. (10) R0 Number 2.4 1.4–3.0 Range of estimates from modelling studies of outbreaks within and outside China, and on the Diamond Princess cruise ship. (20)– (24) The lower bound was based on the lower bound estimate of R0 from the World Health Organization report of outbreaks in China. (25) Systematic review and meta-analysis of studies of R0 suggest that R0 estimates have stablized in the range of 2–3 in more recent studies. (26) Our default estimate of 2.4 was consistent with the assumption used in other modelling studies. (27) Incubation period Days 5.2 3–9 Pooled analysis of 181 confirmed cases with identifiable exposure and symptom onset estimated a median incubation of 5.2 days. (28) We further extracted point (mean or median) estimates of incubation period from a list identified of studies in China and Singapore to inform the range estimates. (20), (29)– (38) Duration of latent infection Days 2 1–3 Assumption based on the relatively short incubation period (5.2 d) and serial interval (4.4 d) of COVID-19; other models have used a latent period of 3 days. (39) Duration of subclinical infectiousness Days 3 2–6 Calculated as the difference between incubation period and latent period (Appendix 1, available at www.cmajopen.ca/content/8/3/E593/suppl/DC1). Duration of symptomatic infectiousness Days 7 5–10 Based on duration of upper respiratory tract viral shedding among individuals with symptoms. (40) Serial interval Days NA 3.1–7.5 No default estimate was used, as serial interval was not used as an input parameter; only the range estimates were used for internal parameter validation (detailed in the Methods section). (20), (38), (41), (42) Initial seeding % of total population 0.0032 0.0011–0.0048 Assumption on range based on detecting 3 travel-related cases by Feb. 23, 2020, at a time when testing criteria was limited to travel to China or contact with a person already diagnosed with COVID-19, (43) and likelihood of detection of imported cases between 11% and 40%. (44) We assumed seeding includes imported cases from outside Canada, between provinces and local transmission that had remained undetected. Clinical Proportion diagnosed with COVID-19 who required admission to hospital % 10 6–20 As of Mar. 23, 10% of confirmed cases in Canada were admitted to hospital. (45) Data on 55 924 confirmed cases in China suggested that 19.9% of confirmed cases were severe, including 6.1% in critical conditions. (34) We therefore assumed that a range from 6% to 20% of detected cases would require admission to hospital in the GTA. Subsequently, Toronto Public Health reported 18 (6.4%) cases admitted to hospital out of 280 confirmed cases of COVID-19 as of Mar. 24. (46) Proportion infected with SARS-CoV-2 who were diagnosed % NA 41–69 Proportion infected who were diagnosed was not directly used as an input parameter, but was used indirectly to calculate the proportion infected who required admission to hospital (detailed below). Analyses on data from China as well as on Japanese citizens returning on repatriation flights showed that 31%–59% of infected cases may not be detected because of asymptomatic infections or mild symptoms. (47)– (49) We therefore assumed a default estimate of 55% (midpoint of the range) for proportion of infected cases that were detected. Proportion infected with SARS-CoV-2 who required admission to hospital % 5.5 2.4–14 We calculated the proportion of infected individuals who require admission to hospital using the proportion of detected cases that require admission to hospital, and multiplied by the proportion of infected cases that may be detected. Proportion admitted to hospital who require ICU care % 33 30–52 As of Mar. 25, 33% of cases admitted to hospital in the Toronto Public Health Unit required ICU admission. (46) Similarly, as of Mar. 23, 40% of cases admitted to hospital in Canada required ICU care. (45) Based on data of 55 924 confirmed cases in China, cases with critical conditions, and thus those that may require ICU care, comprise 30% of confirmed cases with severe or critical conditions. (34) Of 1590 patients admitted to hospital across 575 hospitals in China, 254 had severe conditions, and 52% of these required ICU care or invasive ventilation. (30) We did not estimate the proportion of ICU patients among all patients admitted to hospital in China as many patients were admitted for isolation only rather than because of disease severity in the settings of China. Duration of hospital stay Days 12 10–13 Among 1032 patients admitted to hospital, who did not require ICU care across 552 hospitals in China, their median length of hospital stay at the end of study follow-up was 12 (IQR 10–13) days. (31) This estimate was consistent with the estimates on length of hospital stay among discharged patients with COVID-19 (regardless of ICU stay) in China and Europe. (29), (31), (32), (50)– (52) Duration of ICU stay Days 8 5–13 There are limited data on the length of ICU stay before transfer to the medicine ward for post-ICU recovery. Of 23 ICU patients in Wuhan, who were discharged to the medicine ward from the ICU, their median length of stay in ICU was 8 (IQR 5–13) days. (53) Case-fatality proportion among those in ICU care % 38 17–62 Of 1590 patients admitted to hospital across 575 hospitals in China, 131 patients required ICU care or invasive ventilation, and 50 (38%) of these patients died. (30) We also extracted estimates from several studies in China and in Europe regarding the crude mortality among ICU patients, which ranged from 17% to 62%. (31), (34), (51), (52), (54)– (57) Case-fatality proportion among those diagnosed % NA 0.8–4.24 No default estimate was used, as case-fatality proportion among those diagnosed was not used as an input parameter; only the range estimates were used for internal parameter validation (detailed in the Methods section). Our estimates of the case-fatality proportion among those diagnosed were informed by a range of evidence as shown below, accounting for the uncertainty and heterogeneity in estimates by geographic location and age.
As of Mar. 23, 2020, cases were reported in Canada with 23 deaths, indicating a crude case fatality of 1.1%. (45) Using crude age-specific case-fatality among all confirmed cases in China, (58) and adjusted for the age distribution of confirmed cases in Canada as of Mar. 23, (45) we obtained an overall crude case fatality of 2.5% in Canada. Estimates of case-fatality rate among confirmed cases after adjusting for time lag to death ranged from 0.8% in China excluding Hubei province, 3.48% in China overall and 4.24% in other countries and regions. (59) Analyses using data of cases on Diamond Princess cruise ship estimated an infection fatality rate of 0.5% and case fatality rate of 1.1% after adjusting for time lag to death, and standardizing the age to approximate the age distribution among confirmed cases in China. (60)Note: COVID-19 = coronavirus disease 2019, GTA = Greater Toronto Area, ICU = intensive care unit, IQR = interquartile range, NA = not applicable, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
- Table 2:
Prevalent number of baseline* inpatients and inpatients with COVID-19 in non-ICU and ICU beds in 2 acute care hospitals in the Greater Toronto Area by May 6, 2020
Variable Scenario-based projections Observed§ Among selected scenarios† Across 153 constrained epidemics‡ Fast or large Default Slow or small Median Lower quartile Upper quartile SMH non-ICU inpatient beds, n (capacity = 405; non-COVID-19 patients = 399*) Daily prevalent number of non-ICU COVID-19–related inpatients, n 989 156 5 43 9 211 19 Extra absolute number of non-ICU beds needed, n 983 150 0 37 3 205 NA Projected reduction in non-COVID-19, non-ICU inpatients required to remain below bed capacity, and observed reduction§, % NA 38 0 9 1 51 27 SMH ICU inpatient beds (capacity = 71; non-COVID-19 patients = 56*) Daily prevalent number of ICU COVID-19–related inpatients, n 493 55 7 25 5 129 10 Extra absolute number of ICU beds needed, n 478 40 0 10 0 114 NA Projected reduction in non-COVID-19, ICU inpatients required to remain below bed capacity, and observed reduction§, % NA 71 0 18 0 NA 38 SJHC non-ICU inpatient beds (capacity = 407; non-COVID-19 patients = 374*) Daily prevalent number of non-ICU COVID-19–related inpatients, n 865 137 5 38 8 185 39 Extra absolute number of non-ICU beds needed, n 832 104 0 5 0 152 NA Projected reduction in non-COVID-19, non-ICU inpatients required to remain below bed capacity, and observed reduction§, % NA 28 0 1 0 41 20 SJHC ICU inpatient beds (capacity = 32; non-COVID-19 patients = 18*) Daily prevalent number of ICU COVID-19–related inpatients, n 130 15 2 6 1 34 7 Extra absolute number of ICU beds needed, n 116 1 0 0 0 20 NA Projected reduction in non-COVID-19, ICU inpatients required to remain below bed capacity, and observed reduction§, % NA 6 0 0 0 NA 50 Note: COVID-19 = coronavirus disease 2019, ICU = intensive care unit, NA = not applicable when number of COVID-19–related patients exceeded the hospital capacity, SJHC = St. Joseph Health Centre, SMH = St. Michael’s Hospital.
↵* The baseline number of non-COVID-19 patients was estimated using the median daily number of inpatients on May 30 between 2014 and 2019 in each hospital.
↵† The fast or large epidemic and slow or small epidemic were selected as the upper and lower quartiles of peak incidence, respectively, within the first 300 days from Feb. 23, 2020. The default scenario reflected the default parameter set as shown in Table 1.
↵‡ Among 200 simulated epidemics, 153 met the constraints using the observed data for Lombardy, Italy, and Hong Kong, China, to constrain the simulated epidemics.
↵§ Observed reduction is based on the actual change in inpatient census between the median (generated from pre-COVID-19 years 2014–2019) and observed cases by May 6, 2020.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


