


Article Figures & Tables
Figures
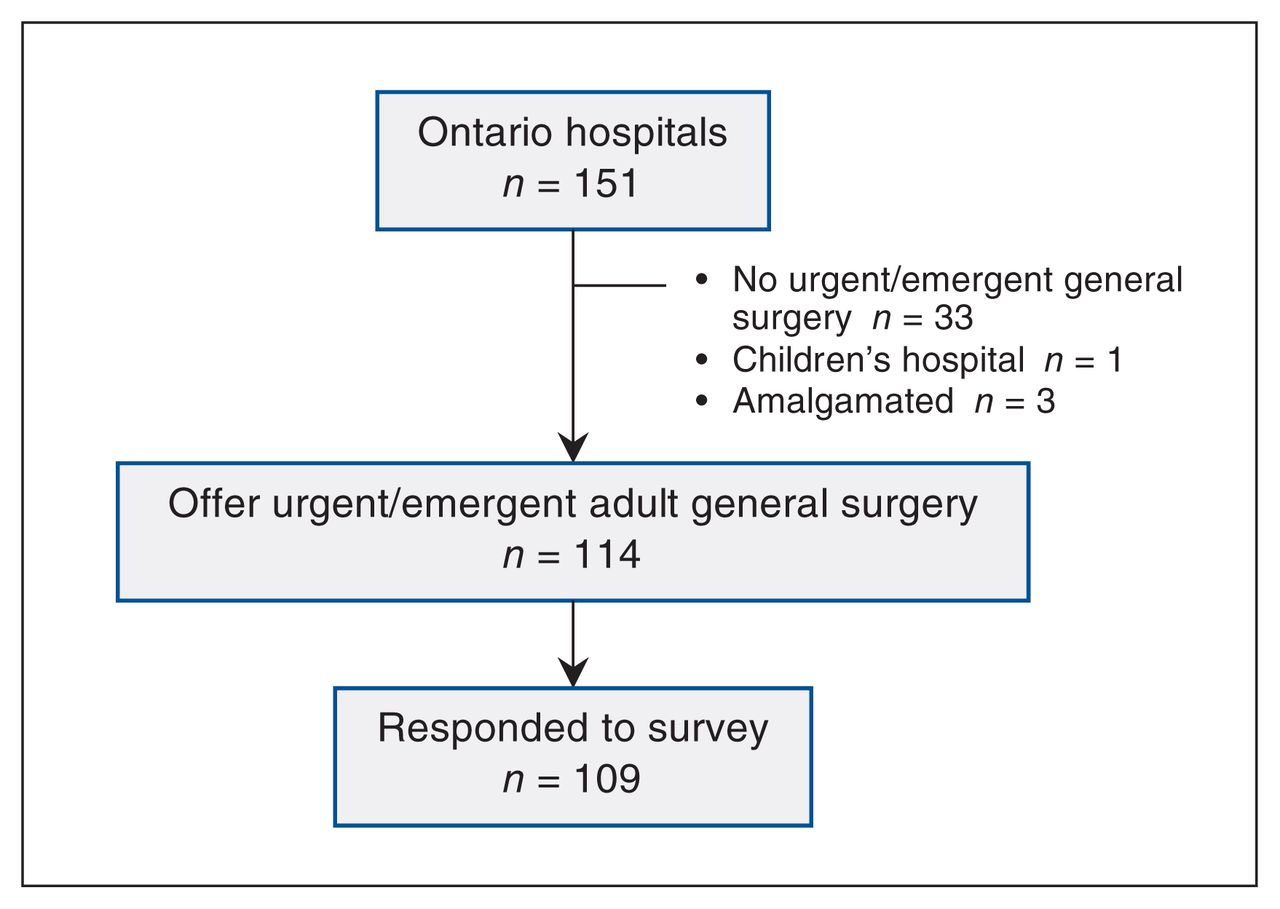
- Figure 1:
Hospital identification and study enrolment.
- Figure 2:
Date of adoption of an emergency general surgery model. Emergency general surgery models in Ontario have been adopted increasingly over time. Newly established emergency general surgery programs (blue) have been counted and plotted for each time period. The cumulative total of Ontario hospitals with an emergency general surgery program (green) has been calculated for the end date of each time period.
- Figure 3:
Dedicated operating room time for emergency general surgery. Eighteen respondents reported the number of operating room hours they provide each week for emergency general surgery. Findings are displayed for academic hospitals (those classified as teaching hospitals by the Ministry of Health) and nonacademic hospitals (those not classified as teaching hospitals by the Ministry of Health). Academic hospitals provided an average of 22.4 hours per week of operating room time; nonacademic hospitals provided an average of 15.6 hours per week. The middle line represents the median, and the boxplot represents the interquartile range.



Tables
Respondent characteristic No. (%) of respondents Large academic
n = 18Large nonacademic
n = 47Small nonacademic
n = 44Respondent role Chair of emergency general surgery 1 (5.6) 0 (0) 0 (0) Chair of general surgery division 10 (55.6) 7 (14.9) 0 (0) General surgeon† 4 (22.2) 15 (31.9) 1 (2.3) Chief of surgery 3 (16.7) 3 (6.4) 3 (6.8) Chief of staff 0 (0) 18 (38.3) 21 (47.7) Manager of perioperative services (or equivalent) 0 (0) 4 (8.5) 19 (43.2) Respondent gender (self-reported) Male 11 (61.1) 26 (55.3) 21 (47.7) Female 7 (38.9) 21 (44.7) 23 (52.3) ↵* Hospitals were categorized as large academic hospitals with more than 100 beds that the Ministry of Health classifies as teaching hospitals, large nonacademic hospitals with more than 100 beds that the Ministry does not classify as teaching hospitals, or small nonacademic hospitals with fewer than 100 beds that the Ministry does not classify as teaching hospitals.
↵† Participation in the emergency general surgery on-call schedule.
Resource No. (%) of hospitals Large academic
n = 18Large nonacademic
n = 47Small nonacademic
n = 44Overall
n = 109EGS
n = 15Non-EGS
n = 3EGS
n = 19Non-EGS
n = 28EGS
n = 3Non-EGS
n = 41EGS
n = 37Non-EGS
n = 72Organizational structure and staffing All surgeons in on-call schedule 6/15 (40.0) 0/2 (0) 14/18 (77.8) 10/20 (50.0) 3/3 (100.0) 7/14 (50.0) 23/36 (63.9) 17/36 (47.2) Other clinical responsibilities 7/15 (46.7) 0/1 (0) 5/17 (29.4) 11/19 (57.9) 3/3 (100.0) 9/18 (50.0) 15/35 (42.9) 20/38 (52.6) Clinical associates 4/15 (26.7) 0/1 (0) 3/17 (17.6) 2/20 (10.0) 0/3 (0) 0/20 (0) 7/35 (20.0) 2/41 (4.9) Residents or fellows 15/15 (100.0) 0/1 (0) 11/17 (64.7) 9/21 (42.9) 0/3 (0) 1/22 (4.5) 26/35 (74.3) 10/44 (22.7) Nurse practitioners or physician assistants 8/15 (53.3) 0/1 (0) 5/18 (27.8) 3/21 (14.3) 0/3 (0) 0/22 (0) 13/36 (36.1) 3/44 (6.8) Outpatient clinic 8/15 (53.3) 0/1 (0) 6/18 (33.3) 0/21 (0) 0/3 (0) 1/22 (4.5) 14/36 (38.9) 1/44 (2.3) Operating room availability Operating room 24/7 14/15 (93.3) 2/3 (66.7) 18/18 (100.0) 22/26 (84.6) 2/3 (66.7) 19/37 (51.4) 34/36 (94.4) 43/66 (65.1) Dedicated operating room time 10/15 (66.7) 0/2 (0) 13/18 (72.2) 0/25 (0) 0/3 (0) 0/35 (0) 23/36 (63.9) 0/62 (0) ASA ≥ 3 15/15 (100.0) 2/3 (66.7) 17/18 (94.4) 22/25 (88.0) 2/3 (66.7) 13/36 (36.1) 34/36 (94.4) 37/64 (57.8) Interventional radiology and interventional endoscopy availability Emergency department 24/7 15/15 (100.0) 3/3 (100.0) 18/18 (100.0) 25/26 (96.2) 3/3 (100.0) 36/38 (94.7) 36/36 (100.0) 64/67 (95.5) Computed tomography 24/7 15/15 (100.0) 2/3 (66.7) 16/17 (94.1) 18/26 (69.2) 2/3 (66.7) 12/37 (32.4) 33/35 (94.3) 32/66 (48.5) Interventional radiology 15/15 (100.0) 1/3 (33.3) 16/18 (88.9) 11/26 (42.3) 0/3 (0) 4/37 (10.8) 31/36 (86.1) 16/66 (24.2) Endoscopy 15/15 (100.0) 2/3 (66.7) 18/18 (100.0) 18/26 (69.2) 2/3 (66.7) 17/37 (45.9) 35/36 (97.2) 37/66 (56.1) ERCP 15/15 (100.0) 0/3 (0) 14/18 (77.8) 11/26 (42.3) 1/3 (33.3) 2/37 (5.4) 30/36 (83.3) 13/66 (19.7) Intensive care unit availability and staffing Intensive care unit 15/15 (100.0) 3/3 (100.0) 17/17 (100.0) 22/25 (88.0) 1/3 (33.3) 17/37 (45.9) 33/35 (94.3) 42/63 (66.7) Intensive care unit step-down 9/15 (60.0) 2/3 (66.7) 8/17 (47.1) 8/25 (32.0) 2/3 (66.7) 7/37 (18.9) 19/35 (54.3) 17/63 (27.0) Intensive care unit outreach team 15/15 (100.0) 3/3 (100.0) 16/17 (94.1) 19/25 (76.0) 1/3 (33.3) 11/37 (29.7) 32/35 (91.4) 33/63 (52.4) Regional participation Transfers to receiving hospital 2/15 (13.3) 1/3 (33.3) 7/17 (41.2) 15/26 (57.6) 2/3 (66.7) 32/37 (86.5) 11/35 (31.4) 48/64 (75.0) Accepts transfers 15/15 (100.0) 1/3 (33.3) 16/17 (94.1) 17/26 (65.4) 1/3 (33.3) 12/37 (32.4) 32/35 (91.4) 30/64 (46.9) Note: ASA = American Society of Anesthesiologists physical classification, (30) EGS = emergency general surgery, ERCP = endoscopic retrograde cholangiopancreatography.
↵* Hospitals are broken down into 3 categories: large academic hospitals with more than 100 beds that the Ministry of Health classifies as teaching hospitals, large nonacademic hospitals with more than 100 beds that the Ministry does not classify as teaching hospitals, or small nonacademic hospitals with fewer than 100 beds that the Ministry does not classify as teaching hospitals.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools


