


Article Figures & Tables
Figures
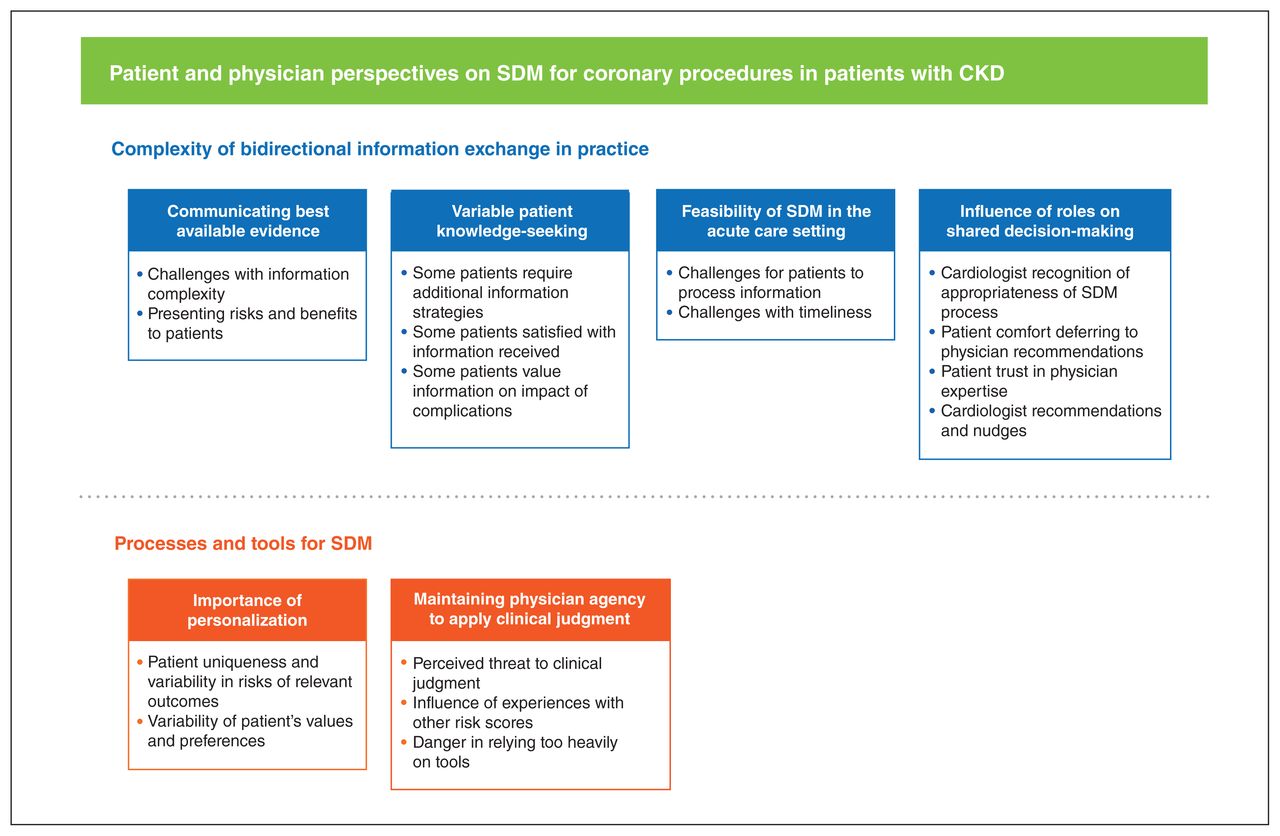
- Figure 1:
Major themes and subthemes identified from analysis of interviews with patients and physicians. Note: CKD = chronic kidney disease, SDM = shared decision-making.

Tables
- Table 1:
Characteristics of patients (n = 20) with acute coronary syndrome or cardiac catheterization in the preceding year*
Characteristic No. (%) of patients† Age, yr Mean ± SD 65.2 ± 11.4 Range 42–83 Sex Male 15 (75) Female 5 (25) Previous consults with a cardiologist Yes 16 (80) No 4 (20) Frequency of previous cardiology visits Not at all 4 (20) Less than once per year 5 (25) Once per year 7 (35) More than once per year 4 (20) Previous consult with a nephrologist Yes 14 (70) No 6 (30) Frequency of previous nephrology visits Not at all 6 (30) Once per year 5 (25) More than once per year 9 (45) Years with kidney disease < 5 6 (30) 5–10 5 (25) ≥ 10 4 (20) Not aware of kidney disease 5 (25) Acute kidney injury requiring dialysis Yes 4 (20) No 16 (80) Theme or subtheme Illustrative quotes Complexities of bidirectional information exchange Communicating best available evidence Challenges with information complexity The discussion about invasive versus medical management is a difficult discussion, and it’s often quite difficult for the patients to understand why you would proceed with medical management as opposed to why would you just open up if there is a narrowing there? That is often hard to communicate to the patient. (Physician 1) I think it’s important to involve the patient, but I think it may become overwhelming for the majority of my elderly patients in particular. (Physician 5) It’s a really complex question because patients present in such a wide variety of situations, so a lot depends on the acuity with which they come in. (Physician 6) I was told at some point earlier, either I read it or I was told … that an angiogram would be destructive to my kidneys. … and I had a choice: fix my heart, kill my kidneys, and live; not fix my heart and not live. (Patient 4) Presenting risks and benefits to patients I don’t usually give the patient numbers … you have an X percent chance of ending up on dialysis. I usually will quote them a high, medium, or low risk of both needing dialysis acutely, as well as acute or permanent injury to their kidney, and then another risk for their need for long-term dialysis. (Physician 5) In terms of patients with kidney disease, then the way I present it depends on what your GFR is before you go, but there is a risk. (Physician 8) I don’t remember being told there would be any risks. It was just, my thought was just do what you need to do. I don’t look at that as a risk or anything like that. Like you’ve got to know what’s wrong with it in order to fix it. (Patient 2) It would have been more appropriate to have had that information from the cardiologist. I went through a bunch of tests and if at some point along that continuum, I had received a “you may need an angiogram and you have chronic kidney disease and here are the implications, be ready.” (Patient 9) Variable patient knowledge-seeking Some patients require additional information strategies There would absolutely be people who would benefit from that, no question, and there will absolutely be people who won’t benefit from that. It’s not just about the information, right, it’s about getting the desired information to the right frame. (Physician 7) The issue for me is I wasn’t psychologically prepared for dialysis, so it came on, even though I intellectually knew it was going to happen someday, I wasn’t anticipating it right away. (Patient 1) Because the psychological effect of going in there with all the follow-up appointments and all the issues that came up because of my kidney, I think it just makes sense to have all the information available before. You know, I was a tough case because you don’t think it will happen to you, but it does and you have to live with it and, you know, I think I made the right decision. But being provided with more information is always better for everyone who’s going through this issue. (Patient 18) Some patients satisfied with information provided I mean, I got all the information I needed and that pretty much ruled out everything … and then just went from there. (Patient 7) I can’t think of anything that would have, I can’t really think of anything that I needed to know that I didn’t know. I was very satisfied with the explanations that were given to me. (Patient 15) Some patients value more information on impact of complications The only thing: more information on possibilities, the risks. (Patient 18) I would have loved to know if there was going to be any effects, specifically because it is such a serious procedure. I would have liked to know if there was going to be an impact. But no, I was not provided that information. (Patient 19) Maybe a pre-op meeting to discuss other instances of things that could go wrong in the procedure, and other things that could happen like kidney disease. I think it’s really important to inform people on specifically what every possible situation that could come out from you having it. (Patient 16) Feasibility of shared decision-making in the acute care setting Challenges for patients to process information Inability to process the information. When you are presenting information in that setting, they may completely forget that it was ever offered to them or it may appear as a kind of barrier or a wall. … It has to be scaled right. (Physician 2) I mean it partly comes down to peoples’ personalities. Some people need more time to digest stuff than other people. So you have to give the patients the opportunity to ask questions, and time to digest the information. (Physician 9) I guess I was sick, I don’t remember. I assume they asked me about it and I told them to go ahead because if I needed a stent or something then they would do it at that time I guess — angioplasty or something. I don’t know. I was so sick, I don’t remember. (Patient 6) Feasibility of shared decision-making in the acute care setting Challenges with timeliness I can see that sometimes things are delayed … . And, if the patient needs more information and needs more discussion time … then that takes a lot more of your time … . But, it could also lead to them perceiving that things took a lot longer … . And then there is always the risk of an adverse event occurring while you are trying to decide whether or not you want to do something or not. (Physician 4) That decision was likely made by the emergency department attendants at the time. It wasn’t made by me. … but I do recall him informing me of the situation, what was happening, and what their plan of attack was. It wasn’t as though they just did it without any kind of consultation with me. (Patient 10) The situation was an emergency. There wasn’t a lot of time to make decisions you know. You don’t have the option or the luxury or the benefit of having a lot of time to make different decisions. (Patient 14) Influence of roles on shared decision-making Cardiologist recognition of appropriateness of shared decision-making process I will always come with what my preference is and sometimes it is a true 50/50, but ultimately the decision is the patient’s to make. (Physician 4) I think information is power for the patients. (Physician 8) Patient comfort deferring to physician recommendations I didn’t really make the decision, but the big thing is, wouldn’t you do it if you knew you could live longer? Even though I was worried that my kidneys could get damaged. The possibility of extending my own life was a bigger priority. (Patient 8) So they more or less did what was necessary and I just went along with it. (Patient 12) All of a sudden I’m flying out to Calgary to take a look at my heart and going through the same thing I saw my dad go through … . I guess I’m relying on the doctors 100% and the nurses and all the medical staff. (Patient 16) Actually my doctor told me it is the best way to know and I just wanted the best care. (Patient 12) Patient trust in physician expertise In going through all of this process, and explaining these aspects, what it does is that it creates a situation of trust, I think, between the patient and the physician. So as you get to those grey areas that are really harder for the patient to understand, they are more willing to trust your interpretation. … And they are always judging your perception versus theirs and back and forth of testing that. And when you get to those grey areas ... you want to first know that you can trust the guy who is giving you advice. (Physician 2) When you are having a heart attack or when you’ve had a heart attack and you are in the hospital, you trust the doctors and whatever the procedure they feel would be the way to go to help you; you know, you go along with it because you don’t know any better … . when they decide that an angiogram was a good idea, well I just thought OK, let’s do it. (Patient 16) Doctor’s suggestion. I believe he’s the expert and he knows better than me. (Patient 20) Cardiologist recommendations and nudges I think if there is a clear-cut benefit one side or the other then I would often try to talk to the patient about risk–benefits, and why we would think that one is of greater benefit than another approach. (Physician 2) After going through with the patient the situation and looking at all the various risks, I would have a conversation with them about the pros and cons of both strategies. I would generally have a recommendation as to which one I feel would be medically the most appropriate, but we would have a conversation about it. (Physician 4) I believe the situation is such that there will be a strong benefit from proceeding, I’m going to present it in that way ... If I think the risk is very high, I’m going to present it that way. If there is some equipoise in the decision, well then the patient’s voice becomes much louder. So when you are at clear ends of the spectrum, you tend to encourage. When you are in the middle, you say OK, what do you think about this? Then their feelings about it become much more important because my understanding of the benefit is less clear. (Physician 9) I always tell the patients, I’m going to give you the information, I’m also going to tell you what I think you should do … If I don’t offer an opinion I’m not sure how useful I am to them. So I give them the information, I tell them what I think they should do based on the relative risks of the 2 options. (Physician 10) Well, he just explained that this was probably the best route to go or to at least to rule out some other things, whatever he thought and that was it. (Patient 5) Yeah, at that time from what I can recall, the doctor just basically said this is what the best procedure is to get the most accurate information from your heart and what it’s doing and that was it. (Patient 13) Processes and tools for shared decision-making Importance of personalization Patient uniqueness and variability in risks of relevant outcomes Everybody comes in very uniquely and everyone’s a complete individual. Like, there’s not a cookbook recipe for everyone in general. (Physician 3) It’s kind of multifactorial things that go into my head when I speak to these patients … it’s not just one thing. (Physician 4) The things that factor into what I would recommend to a patient are the age of the patient … the comorbidities that patient has. (Physician 9) Having a sort of patient information material is often very helpful. Some patient educational materials that might help you frame the conversation might be very helpful. (Physician 6) It also changes depending how bad their renal function is, so obviously if their GFR is 50 I don’t worry about it too much. Whereas if their GFR is near the line of requiring dialysis, I think about it more carefully and I also base that on what their wishes are from their goal of care, would their life be done if they ended up on dialysis and they would never do that. (Physician 8) Variability of patient’s values and preferences For patients who are willing to accept dialysis, should it ever become an issue, we talk a little bit about the lifestyle changes that are going to happen if that becomes necessary. But really the issue for most people is what is their priority? Ultimately they have to decide what they are comfortable with. (Physician 5) I think you have to take into consideration the context. If you have somebody who says — in no way, shape or form I am ever going to agree to dialysis — and you know that you can be speeding that up. Each is unique, and it’s important to have the dialogue with the patient. (Physician 8) Maintaining physician agency and clinical judgment Perceived threat to clinical judgment A lot of physicians, myself included, also don’t want the decision completely taken out of our hands. (Physician 1) I personally don’t use a risk score per se. I evaluate the situation with each patient and determine clinically whether, how high is their risk, basically. (Physician 4) Influence of experiences with other risk scores We use a lot of different risk predictors. So fear would be that people would depend on that and then not use their clinical judgment or look at the patient as a whole anymore … . So could it be helpful? Yes, I think it could be helpful but also think there is room for error and abuse. (Physician 2) Danger in relying too heavily on tools I just wouldn’t want it to become a tool where we stop thinking because the tool says so. Like relying on the tool and stopping to examine the situation ourself, that would be one of the dangers I would see in that. … Well, the only drawback ... I wouldn’t want people to rely only on that tool. (Physician 7) Note: GFR = glomerular filtration rate.
In this issue

{kind=link}
Article tools
Respond to this article


