


Article Figures & Tables
Figures
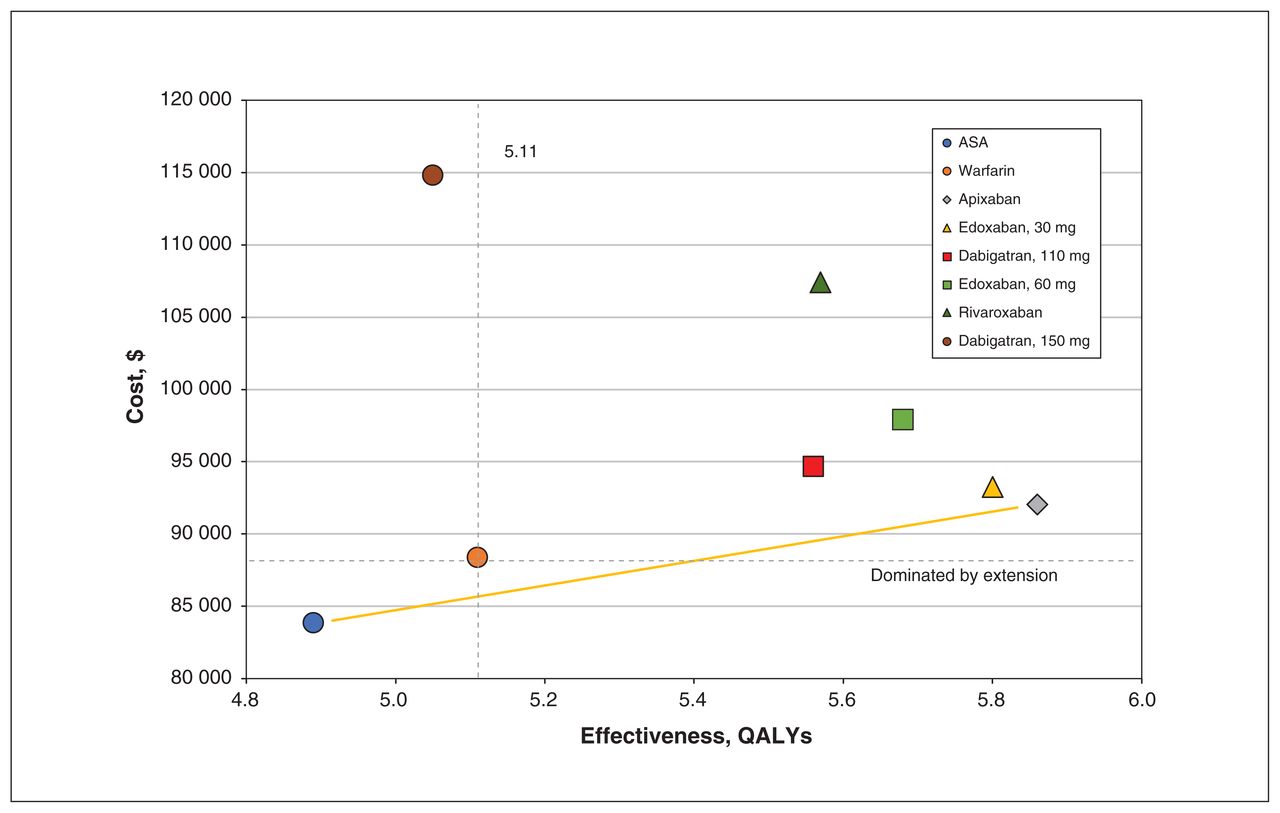
- Figure 1:
Average cost-effectiveness plane. Medications that were lower in cost and higher in effectiveness were more cost-effective. Warfarin was dominated by extension (beige line) by the combination of apixaban and acetylsalicylic acid (ASA). Note: QALY = quality-adjusted life year.
- Figure 2:
Cost-effectiveness acceptability curve for all antithrombotics. The proportion of model iterations in which the drug was most cost-effective reflects residual uncertainty in the model results. Note: ASA = acetylsalicylic acid, QALY = quality-adjusted life year.


Tables
- Table 1:
Baseline characteristics simulated in the health state transition model
Characteristic Value Age, mean ± SD, yr 78.3 ± 5.1 Female sex, % 51 HAS-BLED† CHADS* Low < 3 High ≥ 3 Low < 3 0.58 0.19 High ≥ 3 0.12 0.11 Note: CHADS = congestive heart failure, hypertension, age ≥ 75 yr, diabetes, stroke; HAS-BLED = hypertension, abnormal renal and liver function, stroke, bleeding, labile international normalized ratio, elderly (age > 65 yr), drugs or alcohol (≥ 8 drinks/wk); SD = standard deviation.
↵* Stroke risk score.
↵† Bleeding risk score.
Variable Estimate (range) Distribution Probability First fall 0.32 (0.27 to 0.37) β (14) Subsequent fall 0.58 (0.39 to 0.97) β (14) HR bleed after a fall 1.39 (1.05 to 1.84) Lognormal (24) Any bleed HAS-BLED score high, annual 0.166 (0.111 to 0.221) β (13) HAS-BLED score low, annual 0.091 (0.061 to 0.121) β (13) Major bleed given any bleed 0.31 (0.25 to 0.46) β (25) Intracranial bleed given major bleed 0.21 (0.14 to 0.28) β (26) Bed-bound after intracranial bleed (modified Rankin Scale score ≥ 5) 0.176 (0.117 to 0.235) β (27) Any stroke High CHADS score 0.037 (0.025 to 0.049) Lognormal (28) Low CHADS score 0.083 (0.055 to 0.111) Lognormal (28) Major stroke given stroke 0.41 (0.20 to 0.61) β (29) Bed-bound after major stroke (modified Rankin Scale score ≥ 5) 0.176 (0.117 to 0.235) β (30) OR death due to atrial fibrillation 1.6 (1.2 to 2.2) Lognormal (31) HR death after major stroke 5.29 (3.53 to 7.93) Lognormal (32) HR death after major bleed 3.35 (2.12 to 5.27) Lognormal (32) HR death given bed-bound 3.81 (3.37 to 4.31) Lognormal (33) Cost* Fall, single event 7286.01 (5464.51 to 9107.51) γ (34) Major bleed, initial event 5358.98 (3572.64 to 7145.28) γ (35) Major bleed, monthly 6942.54 (4627.99 to 9255.99) γ (35) Minor bleed, single event 84.38 (55.89 to 111.78) γ (35) Major stroke, initial event 7227.47 (3613.74 to 14 441.79) γ (35) Major stroke, monthly 6476.51 (4384.7 to 8768.31) γ (35) Minor stroke, single event 3613.74 (500.15 to 7227.47) γ (35) Bed-bound (long-term care assumed) 4304.91 (2869.94 to 5739.88) γ (36) Utility/disutility Atrial fibrillation 0.95 (0.93 to 0.98) β (37) Fall, per event† −0.11 (−0.08 to 0.14) β (38) Major bleed, long-term 0.60 (0.40 to 0.80) β (39) Minor bleed, 1 mo† −0.13 (−0.08 to −0.13) β (39) Major stroke, first year 0.26 (0.20 to 0.50) β (39) Major stroke, long-term 0.71 (0.40 to 0.96) β (39) Minor stroke, first year† −0.25 (−0.15 to −0.25) β (39) Bed-bound (modified Rankin Scale score ≥ 5) 0.14 (−0.01 to 0.29) β (37) Note: CHADS = congestive heart failure, hypertension, age ≥ 75 yr, diabetes, stroke; HAS-BLED = hypertension, abnormal renal and liver function, stroke, bleeding, labile international normalized ratio, elderly (age > 65), drugs or alcohol (≥ 8 drinks/wk); HR = hazard ratio; OR = odds ratio.
↵* In 2018 Canadian dollars.
↵† Disutilities.
- Table 3:
Efficacy and cost variables for antithrombotic medications compared to warfarin
Medication Event; OR (95% CI) Cost per month, $* Any bleed Any stroke Death Acetylsalicylic acid (9) 0.59 (0.45 to 0.77) 1.88 (1.40 to 2.51) 1.04 (0.88 to 1.33) 1.02 Apixaban (9) 0.67 (0.60 to 0.75) 0.79 (0.66 to 0.94) 0.88 (0.79 to 0.98) 98.02 Dabigatran, 150 mg (9) 1.56 (0.50 to 5.74) 0.65 (0.52 to 0.81) 0.88 (0.77 to 1.01) 100.32 Dabigatran, 110 mg (9) 0.80 (0.69 to 0.93) 0.90 (0.74 to 1.10) 0.91 (0.80 to 1.04) 100.32 Edoxaban, 60 mg (9) 0.84 (0.77 to 0.90) 0.86 (0.74 to 1.01) 0.86 (0.82 to 1.01) 85.20 Edoxaban, 30 mg (9) 0.59 (0.54 to 0.64) 1.13 (0.97 to 1.32) 0.86 (0.78 to 0.96) 85.20 Rivaroxaban (9) 1.03 (0.95 to 1.11) 0.88 (0.74 to 1.03) 0.83 (0.69 to 1.00) 86.10 Warfarin 1.00 1.00 1.00 39.45‡ Off medication† 0.77 (0.34 to 1.20) 1.47 (1.29 to 1.65) 3.03 (2.79 to 3.27) – Drug Mean (95% credible interval) Cost-effectiveness† Cost, $* Δ Cost QALY Δ QALY ICER Acetylsalicylic acid 83 834 (83 427 to 84 241) – 4.89 (4.88 to 4.90) – – – Warfarin 88 704 (88 268 to 89 140) 4870 (4274 to 5466) 5.11 (5.10 to 5.12) 0.21 (0.21 to 0.23) – Dominated by extension Apixaban, 5 mg 92 056 (91 639 to 92 473) 3352 (2749 to 3955) 5.86 (5.85 to 5.86) 0.74 (0.74 to 0.76) 8517 (7915 to 9121) Cost-effective Edoxaban, 30 mg 93 262 (92 849 to 93 675) 1206 (620 to 1792) 5.80 (5.79 to 5.81) −0.06 (−0.07 to −0.05) – Absolutely dominated Dabigatran, 110 mg 94 670 (94 234 to 95 106) 2614 (2011 to 3217) 5.56 (5.56 to 5.57) −0.29 (−0.30 to −0.28) – Absolutely dominated Edoxaban, 60 mg 97 929 (97 479 to 98 379) 5872 (5260 to 6486) 5.68 (5.68 to 5.69) −0.17 (−0.18 to −0.16) – Absolutely dominated Rivaroxaban, 20 mg 107 425 (106 892 to 107 958) 15 369 (14 692 to 16 046) 5.57 (5.56 to 5.57) −0.29 (−0.30 to −0.28) – Absolutely dominated Dabigatran, 150 mg 114 818 (114 159 to 115 477) 22 761 (21 982 to 23 542) 5.05 (5.04 to 5.06) −0.80 (−0.82 to −0.79) – Absolutely dominated Drug Mean (95% credible interval) Life years* Life expectancy, yr Major stroke, cumulative % Major bleed, cumulative % Time off medication per patient, mo Bed-bound, cumulative % Acetylsalicylic acid 6.25 (6.24 to 6.26) 84.4 (84.4 to 84.5) 26.9 (26.7 to 27.0) 14.2 (14.1 to 14.2) 1.12 (1.12 to 1.13) 5.2 (5.2 to 5.3) Warfarin 6.61 (6.60 to 6.62) 84.7 (84.7 to 84.7) 14.4 (14.4 to 14.5) 25.5 (25.4 to 25.5) 2.04 (2.03 to 2.04) 3.2 (3.2 to 3.2) Apixaban, 5 mg 7.36 (7.35 to 7.37) 85.5 (85.5 to 85.5) 12.9 (12.9 to 13.1) 19.4 (19.4 to 19.5) 1.57 (1.56 to 1.57) 2.7 (2.7 to 2.7) Edoxaban, 30 mg 7.30 (7.29 to 7.30) 85.4 (85.4 to 85.4) 18.4 (18.4 to 18.5) 16.5 (16.5 to 16.6) 1.32 (1.32 to 1.33) 4.0 (4.0 to 4.0) Dabigatran, 110 mg 7.09 (7.09 to 7.10) 85.2 (85.2 to 85.2) 14.1 (14.1 to 14.2) 21.9 (21.9 to 22.0) 1.77 (1.76 to 1.77) 3.0 (3.0 to 3.0) Edoxaban, 60 mg 7.28 (7.28 to 7.29) 85.4 (85.4 to 85.4) 13.8 (13.8 to 13.9) 23.6 (23.6 to 29.3) 1.91 (1.90 to 1.91) 2.9 (2.9 to 2.9) Rivaroxaban, 20 mg 7.30 (7.29 to 7.31) 85.4 (85.4 to 85.4) 14.1 (14.1 to 14.3) 29.2 (29.2 to 29.3) 2.36 (2.35 to 2.37) 3.0 (3.0 to 3.0) Dabigatran, 150 mg 6.91 (6.90 to 6.92) 85.0 (84.9 to 85.0) 9.8 (9.7 to 9.8) 42.7 (42.5 to 43.0) 3.45 (3.43 to 3.47) 2.3 (2.2 to 2.3) ↵* Not adjusted for utility.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.