


Article Figures & Tables
Figures
- Figure 2:
Flow chart showing sampling of facilities and procedures.
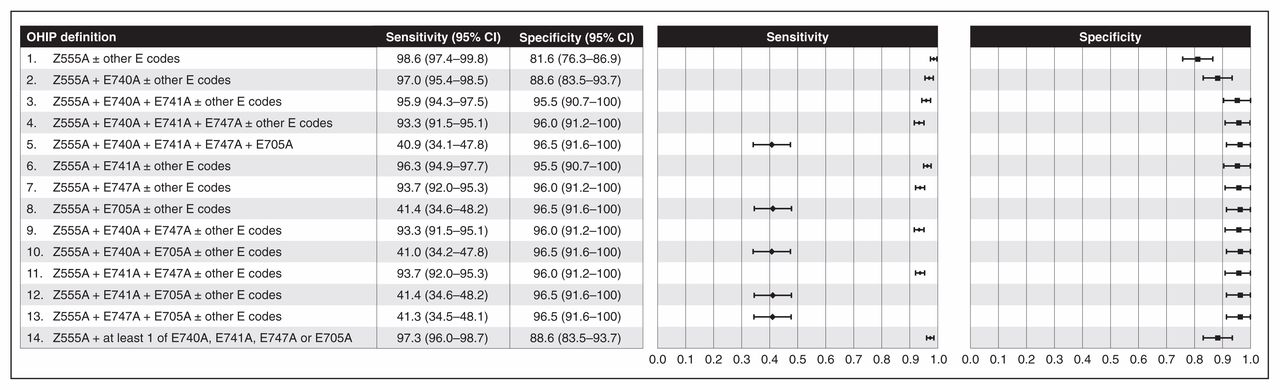
- Figure 1:
Weighted sensitivity and specificity of 14 administrative data definitions using Ontario Health Insurance Plan (OHIP) codes of colonoscopy case compared to the reference standard of colonoscopy intended or performed according to the medical record. Note: CI = confidence interval.
- Figure 3:
Receiver operating curve of the 14 definitions for colonoscopy case. Upper left point of curve corresponds to Ontario Health Insurance Plan (OHIP) definition 6: OHIP codes Z555A + E741A ± other E codes.
- Figure 4:
Sensitivity and specificity of nonhospital setting, colonoscopy completeness, anesthesiologist assistance and polypectomy compared to reference standards. Note: CI = confidence interval, CIHI = Canadian Institute for Health Information, OHIP = Ontario Health Insurance Plan.




Tables
- Table 1:
Description of the cohorts, administrative data definitions and reference standards for 5 colonoscopy data elements
Element Cohort description, size Administrative data definition Reference standard Colonoscopy case All successfully abstracted charts, n = 1845 OHIP codes: Z555A alone or in combination with any of: E740A, E741A, E747A or E705A 14 of the most clinically plausible combinations were evaluated (see Figure 1 for the specific codes included in each definition) Colonoscopy was performed, or there was intent to perform colonoscopy according to endoscopist’s procedure note* Nonhospital clinic Charts in which colonoscopy was intended or performed, n = 1282 OHIP code E649A billed on date of colonoscopy
No record in CIHI database overlapping with date of colonoscopy according to OHIP database (i.e., no record of procedure’s being done in hospital)
OHIP code E649A and no overlapping record in CIHI database
Presence of endoscopist’s procedure note in nonhospital facility chart Anesthesiologist assistance Charts in which colonoscopy was intended or performed, n = 1282 OHIP codes for anesthesia (003C or procedure code with “C” suffix [see supplementary tables, Appendix 1, available at www.cmajopen.ca/content/6/3/E330/suppl/DC1]) billed on date as colonoscopy in same patient Presence of anesthesiologist record in chart regardless of type of sedating agent
Use of propofol as sedating agent according to anesthesiologist’s record†
Colonoscopy completeness‡ Charts in which procedure billed with colonoscopy codes, and colonoscopy or flexible sigmoidoscopy was intended,§ n = 1477 (administrative data definition 1), n = 1016 (administrative data definition 2) OHIP code E747A (to cecum) or E705A (to terminal ileum) billed among colonoscopy procedures defined using most sensitive definition (Z555A ± other E codes)
OHIP code E747A or E705A billed among colonoscopy procedures defined using most accurate definition (Z555A + E741 ± other E codes)
Colonoscopy “intended” and “complete” according to endoscopist’s procedure note Polypectomy¶ Charts in which colonoscopy was intended or performed,** n = 1256 (reference standard 1), n = 1252 (reference standard 2) OHIP code Z571A alone
OHIP code Z571A, Z570A or E685A
OHIP code Z571A, Z570A, E685A or E717A
Polyp visualized or polypectomy described according to endoscopist’s procedure note
Adenoma, advanced adenoma or sessile serrated polyp according to pathologist’s report††
Note: CIHI = Canadian Institute for Health Information, OHIP = Ontario Health Insurance Plan.
↵* Completed by the endoscopist; includes a description of the procedure, including findings.
↵† Completed by the anesthesiologist; record of anesthetic administered during the procedure.
↵‡ Procedures intended as flexible sigmoidoscopy for which E747A or E705A was billed were classified as false-positive. Procedures intended as flexible sigmoidoscopy for which E747A and E705A were not billed were classified as false-negative.
↵§ Excluding those with prior total colectomy or right hemicolectomy.
↵¶ Because the histologic findings of the polyp are not available in administrative databases, we could not define adenoma using these data.
↵** Excluding those with missing data for reference standard.
↵†† Report on the histologic findings of specimens, such as polyps, obtained at colonoscopy.
- Table 2:
Patient and procedure characteristics for all successfully abstracted charts and for charts in which colonoscopy was intended or performed
Characteristic No. (%) of charts* All abstracted charts
n = 1845Colonoscopy intended or performed
n = 1282Age group, yr < 50 469 (25.4) 251 (19.6) 50–59 517 (28.0) 395 (30.8) 60–69 430 (23.3) 327 (25.5) 70–74 174 (9.4) 134 (10.4) > 74 255 (13.8) 175 (13.6) Sex Female 986 (53.4) 709 (55.3) Male 859 (46.6) 573 (44.7) Procedure(s) performed† Colonoscopy only 1143 (62.0) 1125 (87.8) Gastroscopy only 45 (2.4) ≤ 5 Flexible sigmoidoscopy only 432 (23.4) ≤ 5 Colonoscopy + gastroscopy 200 (10.8) 151 (11.8) Flexible sigmoidoscopy + gastroscopy 12 (0.6) ≤ 5 Colonoscopy + other procedure ≤ 5 ≤ 5 Flexible sigmoidoscopy + other procedure ≤ 5 0 (0) Other procedure only 6 (0.3) 0 (0) Median neighbourhood income quintile‡ 1 (lowest) 300 (16.3) 205 (16.0) 2 331 (17.9) 225 (17.6) 3 337 (18.3) 233 (18.2) 4 393 (21.3) 265 (20.7) 5 (highest) 474 (25.7) 348 (27.1) Missing 10 (0.5) 6 (0.5) Setting Nonhospital clinic 284 (15.4) 216 (16.8) Hospital 1561 (84.6) 1066 (83.2) - Table 3:
Positive predictive values of OHIP definition of colonoscopy, nonhospital setting, colonoscopy completeness, anesthesiologist assistance and polypectomy compared to reference standards
OHIP definition PPV (95% CI) Colonoscopy case 1. Z555A ± other E codes 96.4 (95.2–97.6) 2. Z555A + E740A ± other E codes 97.7 (96.6–98.8) 3. Z555A + E740A + E741A ± other E codes 99.1 (98.0–100) 4. Z555A + E740A + E741A + E747A ± other E codes 99.1 (98.1–100) 5. Z555A + E740A + E741A + E747A + E705A 98.3 (96.0–100) 6. Z555A + E741A ± other E codes 99.1 (98.1–100) 7. Z555A + E747A ± other E codes 99.2 (98.1–100) 8. Z555A + E705A ± other E codes 98.3 (96.0–100) 9. Z555A + E740A + E747A ± other E codes 99.1 (98.1–100) 10. Z555A + E740A + E705A ± other E codes 98.3 (96.0–100) 11. Z555A + E741A + E747A ± other E codes 99.2 (98.1–100) 12. Z555A + E741A + E705A ± other E codes 98.3 (96.0–100) 13. Z555A + E747A + E705A ± other E codes 98.3 (96.0–100) 14. Z555A + 1 or more of E740A, E741A, E747A or E705A 97.7 (96.6–98.8) Nonhospital setting 1. E649A billed on date of colonoscopy 100 (100–100) 2. No record in CIHI database overlapping with date of colonoscopy according to OHIP database 100 (100–100) 3. E649A and no overlapping record in CIHI database 100 (100–100) Colonoscopy completeness, defined using most sensitive colonoscopy definition 1. Weighted analysis results 99.0 (98.3–99.7) 2. Unweighted analysis results 99.0 (98.3–99.7) Colonoscopy completeness, defined using most accurate colonoscopy definition 1. Weighted analysis results 99.0 (98.3–99.7) 2. Unweighted analysis results 99.0 (98.3–99.7) Anesthesiologist assistance 1. v. “anesthesiologist’s record” 83.8 (71.5–96.0) 2. v. “use of propofol” 77.2 (64.3–90.1) Polypectomy v. “polyp seen or removed” 1. Z571A alone 99.0 (97.7–100) 2. Z571A, Z570A or E685A 98.7 (97.3–100) 3. Z571A, Z570A, E717A or E685A 79.2 (74.3–84.2) v. “histology” 1. Z571A alone 68.1 (62.2–74.1) 2. Z571A, Z570A or E685A 64.1 (58.1–70.2) 3. Z571A, Z570A, E717A or E685A 49.7 (44.4–55.0) Note: CI = confidence interval, CIHI = Canadian Institute for Health Information, OHIP = Ontario Health Insurance Plan, PPV = positive predictive value.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.