


Article Figures & Tables
Figures
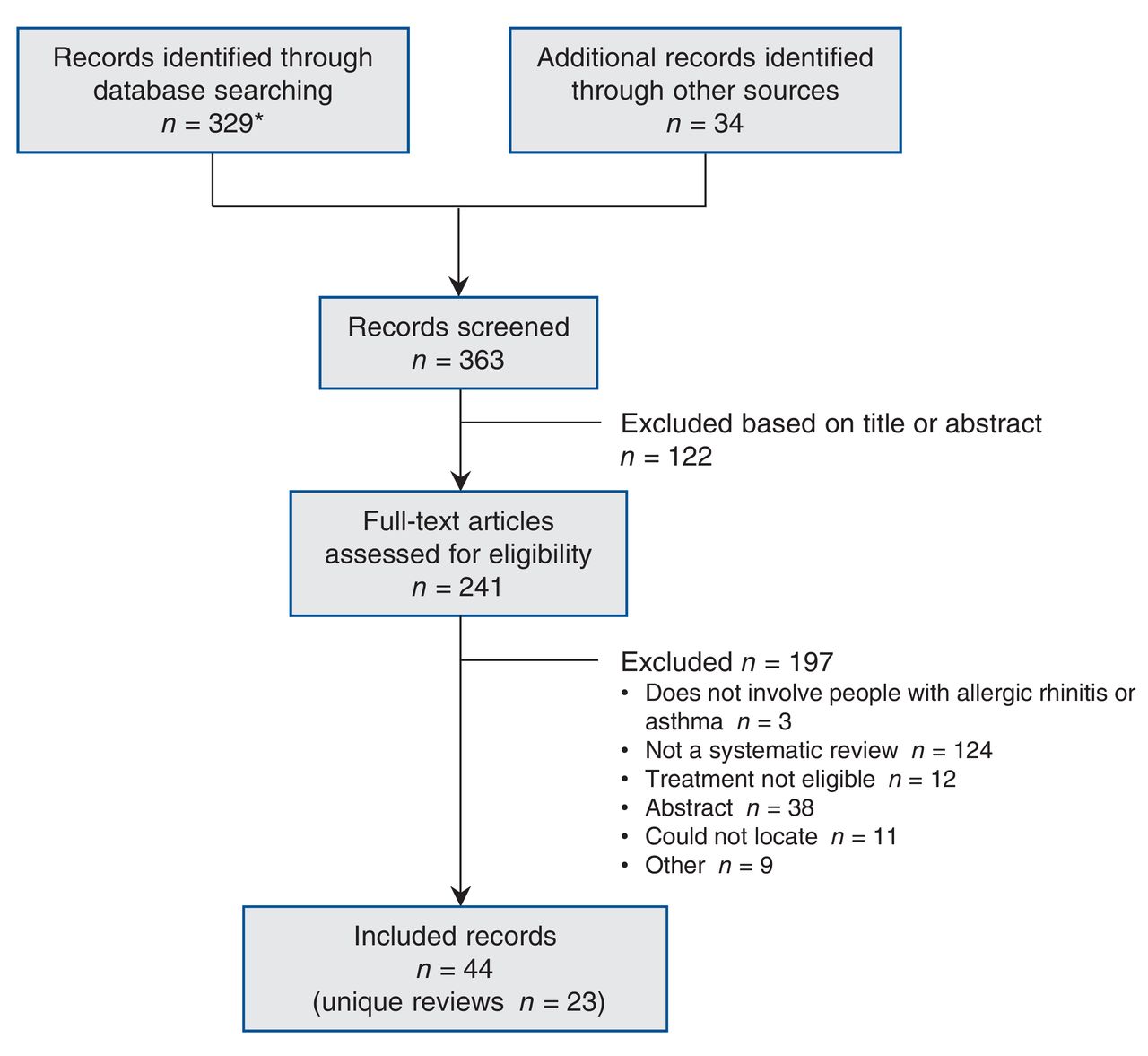
- Figure 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram showing selection of included reviews. *The initial search results included studies on venom immunotherapy, which was subsequently determined to be outside the scope of this overview. Venom immunotherapy was assessed in the environmental scan portion of this drug class review (http://odprn.ca/wp-content/uploads/2016/02/Allergen-Immunotherapy_Environmental-Report_Oct-2-2015_FINAL.pdf).
- Figure 2
Summary of benefits of subcutaneous (SCIT) and sublingual (SLIT) immunotherapy. The five contiguous circles correspond, respectively, to the 5 efficacy outcomes: total combined symptom-medication score, symptom score, medication score, disease-specific quality of life and adherence/discontinuation. A green circle indicates that immunotherapy is significantly better than placebo, a red circle indicates that immunotherapy is significantly worse than placebo, a grey circle indicates that there is no significant difference between immunotherapy and placebo, and a white circle indicates that the outcome was not available for analysis. In cases of immunotherapy versus immunotherapy, significance is reported relative to the first agent listed in the heading.


Tables
Condition; author Search date Country No. of included studies Included design Population
(adult or children)Duration Indication Immunotherapy evaluated Type of analysis Included allergens AMSTAR score* Allergic asthma Liao et al.,16 2015 February 2014 China 11 RCT Children 4 mo-3 yr AA SLIT Meta-analysis House dust mite 7 Normansell et al.,17 2015 March 2015 UK 52 RCT Mixed 1 d-3 yr AA ± AR SLIT Meta-analysis House dust mite, grass pollen, birch pollen, cockroach, cat, Alternaria, Parietaria, Artemisia, olive pollen 11 Lu et al.,18 2015 February 2013 China 19 RCT Mixed 4 mo-3 yr AA SCIT Meta-analysis House dust mite 7 Tao et al.,19 2014 March 2012 China 16 RCT Mixed 10 wk- 25 mo AA ± AR ± conjunctivitis SLIT Meta-analysis House dust mite, grass, birch pollen 6 Abramson et al.,1 2010 August 2005 Australia 88 RCT Mixed ≤ 3 yr AA SCIT Meta-analysis House dust mite, pollen, animal dander, mould, latex 7 Allergic rhinitis Yang et al.,20 2016 April 2016 China 4 RCT Mixed 7-20 mo AR SLIT Meta-analysis Cedar pollen 7 Di Bona et al.,21 2015 April 2014 Italy 13 RCT Mixed 12 wk-1 yr AR ± AA SLIT Meta-analysis Grass pollen 8 Seidman et al.,3 2015 November 2013 US 267 CPG, SR, RCT Mixed NR Seasonal and perennial AR SCIT, SLIT Narrative NR 0 CADTH,22 2014 June 2014 Canada 8 RCT Mixed 9 wk-2 yr Seasonal AR ± conjunctivitis SCIT, SLIT Network meta-analysis Grass pollen 7 Feng et al.,23 2014 May 2013 China 9 RCT Mixed 2.3 mo-3 yr AR SCIT (cluster) Meta-analysis Grass pollen, cat hair 8 Devillier et al.,24 2014 2013; mo NR France 28† RCT Mixed NR Seasonal AR SLIT Meta-analysis Grass pollen 5 Dranitsaris et al.,25 2014 December 2012 Canada 20 RCT Mixed 1-34 mo Seasonal AR SCIT, SLIT Meta-regression Grass pollen 3 Larenas-Linnemann et al.,26 2013 December 2012 Mexico 28 RCT, NRS Children, adolescents 6 mo-3 yr AR or RC ± AA SLIT Narrative Grass or tree pollen, house dust mite, Alternaria, peanut, milk 6 Lin et al.,27 2013 (Kim et al., 2013, Erekosima et al., 2014, Lin et al., 2013, Chelladurai et al., 2013) May 2012 US 142‡ RCT Mixed NR Allergic RC ± AA SCIT, SLIT Narrative Pollen, cat, dog, cockroach, house dust mite 11 Manzotti et al.,28 2013 January 2012 Italy 7 RCT Mixed 5.3-7 mo Seasonal allergic RC SLIT Narrative Grass pollen 1 Meadows et al.,29 2013 (Dretzke et al., 2013) April 2011 UK 28 RCT Mixed Mean 3.6 yr AR ± AA SCIT, SLIT Meta-analysis Grass, tree or ragweed pollen, Alternaria, Parietaria 10 Calderón et al.,6 2013 March 2013 UK 44 RCT Mixed 6-28 mo AR and AA SCIT, SLIT Narrative House dust mite 3 Purkey et al.,30 2013 December 2011 US 12 RCT NR ≤ 5 yr Seasonal and perennial AR SCIT, SLIT Narrative Pollen 3 Calderón et al.,31 2011 January 2011 UK 42 RCT Mixed 3-36 mo Seasonal and perennial ARC or conjunctivitis SLIT Meta-analysis Pollen 11 Larenas-Linnemann et al.,32 2011 April 2011 Mexico 31§ RCT, NRS Children and adolescents 3-36 mo Seasonal or perennial AR or RC ± AA SCIT Narrative House dust mite, grass pollen, birch, fungus 5 Radulovic et al.,33 2010 (Wilson et al., 2009) August 2009 UK 60 RCT Mixed 2 wk-3 yr¶ Seasonal and perennial AR SLIT Meta-analysis Parietaria, ragweed, tree pollen, house dust mite, cat 10 Bousquet et al.,2 2011 June 2009 France 94 RCT Mixed NR AR conjunctivitis, ± AA SCIT, SLIT Narrative Grass pollen 2 Calderón et al.,34 2010 January 2009 UK 33 RCT Mixed 1-84 mo Seasonal ARC SCIT, SLIT Narrative Grass pollen 1 Note: AA = allergic asthma, AR = allergic rhinitis, ARC = allergic rhinoconjunctivitis, CADTH = Canadian Agency for Drugs and Technologies in Health, CPG = clinical practice guideline, NR = not reported, NRS = nonrandomized study, RC = rhinoconjunctivitis, RCT = randomized controlled trial, SCIT = subcutaneous immunotherapy, SLIT = sublingual immunotherapy, SR = systematic review, UK = United Kingdom, US = United States.
*Maximum 11.
†Authors reported that 28 publications were included; unclear whether this represents the number of unique RCTs.
‡Authors reported that 142 articles were included; unclear whether this represents the number of unique RCTs.
§Authors reported that 31 articles were included; unclear whether this represents the number of unique RCTs.
¶Three consecutive grass pollen seasons.
- Table 2: Benefits of subcutaneous and sublingual immunotherapy among participants with allergic asthma
Author Population Included allergens Comparison Unadjusted standard mean difference (95% CI); I2; k AMSTAR score* Search date Symptom score Medication score Liao et al.,16 2015 Children with AA House dust mite SLIT v. placebo -1.02(-2.07 to -0.33);92%; 8 -0.52(-1.75 to 0.71);85%; 3 7 February 2014 Normansell et al.,17 2015 AA ± AR House dust mite, grass, pollen, birch pollen, cockroach, cat, Alternaria, Parietaria, Artemisia, olive pollen SLIT v. placebo - - 11 March 2015 Lu et al.,18 2015 AA House dust mite SCIT v. placebo -0.94(-1.58 to -0.29);92%; 13 - 7 February 2013 Tao et al.,19 2014 AA ± AR and/or conjunctivitis House dust mite, grass, birch pollen SLIT v. placebo -0.74(-1.26 to -0.22);91%; NR -0.78(-1.45 to -0.11);93%; NR 6 March 2012 Abramson et al.,1 2010 AA House dust mite, pollen, dander, mould, latex SCIT v. placebo -0.59(-0.83 to -0.35);73%; 34 - 7 August 2005 Note: AA = allergic asthma, AR = allergic rhinitis, AMSTAR = Assessing the Methodological Quality of Systematic Reviews, k = number of included studies, NR = not reported, SCIT = subcutaneous immunotherapy, SLIT = sublingual immunotherapy.
*Maximum 11.
- Table 3: Benefits of subcutaneous and sublingual immunotherapy among participants with allergic rhinitis
Comparison; author Population Allergen Unadjusted standard mean difference (95% CI*); I2; k AMSTAR score‡ Search date Total combined symptom-medication score Symptom score Medication score Disease-specific quality of life Treatment discontinuation† SLIT v. placebo Yang et al.,20 2016 AR Cedar pollen -0.94(-1.75 to -0.14);93%; 4 - - - - 6 April 2016 Di Bona et al.,21 2015 ARC Grass pollen - -0.28(-0.37 to -0.19);54%; 13 -0.24(-0.31 to -0.17);22%; 12 - SLIT: 6%,placebo: 2.2% 9 April 2014 Devillier et al.,24 2014 ARC Grass, tree or ragweed pollen Hedges g -0.31(-0.39 to -0.22);NR; 11 - - - - 5 2013§ Dranitsaris et al.,25 2014 (Oralair) AR Grass pollen - - - - RR 4.88 (2.41 to 9.79); 6 trial arms 3 December 2012 Dranitsaris et al.,25 2014 (Grazax) AR Grass pollen - - - - RR 1.90 (1.21 to 3.00); 8 trial arms 3 December 2012 Meadows et al.,29 2013 AR ± AA Grass, tree or ragweed pollen, Alternaria, Parietaria -0.40(-0.55 to -0.25);39%; 6 -0.33(-0.42 to -0.25);42%; 42 -0.27(-0.37 to -0.17);49%; 35 -0.37(-0.52 to -0.22);59%; 7 - 10 April 2011 Radulovic et al.,33 2010 AR Parietaria, tree or ragweed pollen, house dust mite, cat - -0.49(-0.64 to -0.34);81%; 49 -0.32(-0.43 to -0.21);50%; 38 - - 10 August 2009 SCIT v. placebo Dranitsaris et al.,25 2014¶ AR Grass pollen - -0.30(-0.39 to -0.20);7 trial arms - - RR 3.16 (1.40 to 7.10); 7 trial arms 3 December 2012 Meadows et al.,29 2013 AR ± AA Grass, tree or ragweed pollen, Alternaria, Parietaria -0.48(-0.67 to -0.29);22%; 8 -0.65(-0.85 to -0.45);57%; 17 -0.55(-0.75 to -0.34);57%; 16 MD -0.74(-0.92 to -0.56);0%; 8 - 10 April 2011 SCIT v. SLIT¶ Dranitsaris et al.,25 2014 AR Grass pollen - -0.21(-0.36 to -0.07);7 trial arms; favours SLIT - - - 3 December 2012 Meadows et al.,29 2013 AR ± AA Grass, tree or ragweed pollen, Alternaria, Parietaria - SSD 0.35(0.13 to 0.59), favours SCIT;SCIT: 17 trials, SLIT: 42 trials SSD 0.27(0.03 to 0.53), favours SCIT;SCIT: 16 trials, SLIT: 35 trials SSD -0.52(-0.07 to 1.04);SCIT: 8 trials, SLIT: 4 trials - 10 April 2011 Note: AA = allergic asthma, AR = allergic rhinitis, ARC = allergic rhinoconjunctivitis, MD = mean difference, NR = not reported, k = number of included randomized controlled trials, RC = rhinoconjunctivitis, RR = relative risk, SCIT = subcutaneous immunotherapy, SLIT = sublingual immunotherapy, SSD = standardized score difference.
*95% credible interval for indirect treatment comparisons (SCIT v. SLIT).
†Treatment discontinuation, not discontinuation owing to adverse events.
‡Maximum 11.
§Month not reported.
¶Indirect treatment comparisons.
Condition; author Intervention Anaphylaxis Death Allergic asthma Normansell et al.,17 2015 SLIT v. placebo NR "None of the included studies reported any deaths." Calderón et al.,6 2013 SCIT v. placebo "Several serious TEAEs (some of which required epinephrine) were reported. Pichler et al.(56) mentioned use but did not state whether this concerned an active treatment or placebo group participant. The 4 incidents reported by Bousquet et al.(25) (3 of which required epinephrine) all concerned the active treatment group during the rush updosing phase" NR Lu et al.,18 2015 SCIT v. placebo NR NR Abramson et al.,1 2010 SCIT v. placebo "Systemic adverse reactions were reported by 32 studies. Systemic reactions were defined as any of anaphylaxis, asthma, rhinitis or urticaria, or any combination of these. The pooled relative risk was 2.45 (95% CI 1.91 to 3.13) in the 26 reporting reactions per patient and this was relatively homogeneous (I2 = 27%)."Incidence of near-fatal reactions estimated to be 1 per 1 million reactions Incidence of fatal reactions estimated to be 1 per 2.5 million Liao et al.,16 2015 SLIT v. placebo NR NR Calderón et al.,6 2013 SLIT v. placebo "The only serious adverse event (AE) reported was a severe exacerbation of asthma in 1 patient in the placebo group in the study by Pham-Thi et al.(55)" "The only serious adverse event (AE) reported was a severe exacerbation of asthma in 1 patient in the placebo group in the study by Pham-Thi et al.(55)" Tao et al.,19 2014 SLIT v. placebo "The main adverse reactions in our analysis were mild local reactions, such as mouth and/or throat itchiness, redness and swelling. The risk of adverse effects found in our meta-analysis was RR 2.23 (95% CI 1.17 to 4.24; p = 0.01) (Fig. 9). However, Tari et al. reported that severe asthma occurred in three patients attributing to the side effects of SLIT. (22)" NR Allergic rhinitis Calderón et al.,34 2010 SCIT v. placebo "All studies reported a higher proportion of adverse events (AEs) in SIT groups than in placebo groups. Systemic AEs requiring administration of subcutaneous adrenaline were observed. (17, 21)" Both were in SCIT group. NR Calderón et al.,6 2013 SCIT v. placebo "The 2 earliest publications (23, 36) each featured 1 anaphylactic reaction caused by SCIT. More recent trials did not observe anaphylactic reactions." NR Meadows et al.,29 2013 SCIT v. placebo "Post-injection anaphylaxis was reported in only one small trial (159) (total n = 76) but was considerably more frequent following active treatment, occurring in approximately 10 of 39 patients (compared with 1 of 37 receiving placebo); 8 of the 10 patients were treated with adrenaline." NR Lin et al.,27 2013 SCIT v. placebo "Thirteen anaphylactic reactions were reported in four trials." None reported in control group. "No deaths were reported." Purkey et al.,30 2013 SCIT v. placebo "1 episode of anaphylaxis consisting of asthma and pruritus of the ear canal and oropharynx that required administration of epinephrine and oral corticosteroids.""In the patient who experienced anaphylaxis, symptoms developed 1 minute after administration of the 61st dose of treatment. Administration of subcutaneous epinephrine, intravenous methylprednisone, and nebulized salbutamol resulted in rapid resolution of symptoms. SCIT was discontinued in this patient." "Local and systemic reactions (rare but with significant morbidity/mortality if they occur)." Yang et al.,20 2016 SLIT v. placebo NR NR Di Bona et al.,21 2015 SLIT v. placebo No anaphylactic reactions reported in either SLIT or placebo groups. Nine events requiring epinephrine administration were reported in the SLIT group compared with 3 in the placebo group. NR Devillier et al.,24 2014 SLIT v. placebo NR NR CADTH,22 2014 SLIT v. placebo "In studies P05238, P05239, and P08067, it was mentioned that no participants experienced anaphylactic shock, and in studies GT-02, GT-07, GT-08, GT-12, and GT-14, there was no specific mention of anaphylactic shock. No incidence of anaphylaxis was reported in GT-02, GT-07, GT-08, and GT-12. In study P05238, one participant in the PPAE group received epinephrine due to an adverse event that occurred following the first administration of the study drug, and one placebo-treated patient used epinephrine in response to an anxiety attack, which the manufacturer stated was not an indicated (or medically appropriate) use for this medication." "There were no deaths reported in studies GT-07, GT-02, GT-14, GT-12, and P05239. In studies GT-08, P05238, and P08067, one death was reported in each study … none were considered by the manufacturer to be treatment related." Calderón et al.,6 2013 SLIT v. placebo "Bahceciler et al.(22) did not observe any AEs of note with a maintenance dose of 8 mg of 'Der p' allergens in children and adolescents. In contrast, de Bot et al.(31) studied a maintenance dose of 2 mg of Der p 1 allergen and reported that 96% of both active and placebo group patients experienced TEAEs (including a high proportion of nonlocal AEs). Nevertheless, no immunotherapy-dependent serious AEs were reported in any of the active groups." NR Lin et al.,27 2013 SLIT v. placebo "No life-threatening reactions, anaphylaxis, or deaths were reported in these trials." "No life-threatening reactions, anaphylaxis, or deaths were reported in these trials." Meadows et al.,29 2013 SLIT v. placebo "Anaphylaxis was reported in two trials (192, 195) and occurred in 4 of 427 patients receiving active treatment and in none of 282 patients receiving placebo." NR Manzotti et al.,28 2013 SLIT(Grazax or Oralair)v. placebo "However, it seems not advisable to use Grazax, that starts directly with the maintenance dose, in subjects with an history of systemic reactions to SCIT, because anaphylactic reactions at the first dose were reported in such subjects. (21)" NR Radulovic et al.,33 2010 SLIT v. placebo "None of the studies reported anaphylaxis." NR Calderón et al.,34 2010 SLIT drops v. placebo "No life-threatening AEs or fatalities were described." "No life-threatening AEs or fatalities were described." Calderón et al.,34 2010 SLIT tablets v. placebo "All seven studies reported on safety in detail; the principal AEs were mild, local and transient and none required adrenaline administration. Treatment-related SAEs were not observed." "All seven studies reported on safety in detail; the principal AEs were mild, local and transient and none required adrenaline administration. Treatment-related SAEs were not observed." Note: AE = adverse event, CADTH = Canadian Agency for Drugs and Technologies in Health, CI = confidence interval, NR = not reported, RR = relative risk, SAE = systemic adverse event, SCIT = subcutaneous immunotherapy, SLIT = sublingual immunotherapy, TEAE = treatment-emergent adverse event.
*May include both children and adults.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.