


Abstract
Background Tobacco smoking and cannabis use are independently associated with depression, and evidence suggests that people who use both tobacco and cannabis (co-consumers) are more likely to report mental health problems, greater nicotine dependence and alcohol misuse than those who use either product exclusively. We examined prevalence of cannabis use and depressive symptoms among Canadian adults who smoke cigarettes and tested whether co-consumers of cannabis and tobacco were more likely to report depressive symptoms than cigarette-only smokers; we also tested whether cigarette-only smokers and co-consumers differed on cigarette dependence measures, motivation to quit smoking and risky alcohol use by the presence or absence of depressive symptoms.
Methods We analyzed cross-sectional data from adult (age ≥ 18 yr) current (≥ monthly) cigarette smokers from the Canadian arm of the 2020 International Tobacco Control Policy Evaluation Project Four Country Smoking and Vaping Survey. Canadian respondents were recruited from Leger’s online probability panel across all 10 provinces. We estimated weighted percentages for depressive symptoms and cannabis use among all respondents and tested whether co-consumers (≥ monthly use of cannabis and cigarettes) were more likely to report depressive symptoms than cigarette-only smokers. Weighted multivariable regression models were used to identify differences between co-consumers and cigarette-only smokers with and without depressive symptoms.
Results A total of 2843 current smokers were included in the study. The prevalence of past-year, past-30-day and daily cannabis use was 44.0%, 33.2% and 16.1%, respectively (30.4% reported using cannabis at least monthly). Among all respondents, 30.0% screened positive for depressive symptoms, with co-consumers being more likely to report depressive symptoms (36.5%) than those who did not report current cannabis use (27.4%, p < 0.001). Depressive symptoms were associated with planning to quit smoking (p = 0.01), having made multiple attempts to quit smoking (p < 0.001), the perception of being very addicted to cigarettes (p < 0.001) and strong urges to smoke (p = 0.001), whereas cannabis use was not (all p ≥ 0.05). Cannabis use was associated with high-risk alcohol consumption (p < 0.001), whereas depressive symptoms were not (p = 0.1).
Interpretation Co-consumers were more likely to report depressive symptoms and high-risk alcohol consumption; however, only depression, and not cannabis use, was associated with greater motivation to quit smoking and greater perceived dependence on cigarettes. A deeper understanding of how cannabis, alcohol use and depression interact among people who smoke cigarettes is needed, as well as how these factors affect cessation activity over time.
Tobacco smoking is the global leading cause of non-communicable diseases and premature death.1,2 In Canada, 47 000 people die annually from smoking-related diseases.3 There are key disparities between adults who smoke cigarettes and those who do not, including mental health problems and use of other drugs, most notably cannabis.4,5 In particular, evidence shows that people with depression are disproportionately affected by high smoking prevalence and heavier smoking.6,7 The relation between depression and difficulty quitting smoking remains unclear; however, evidence suggests that cigarette smokers with depression are highly motivated to quit smoking8–11 but may be less successful maintaining abstinence.9 For example, Cooper and colleagues assessed data from a large population study of cigarette smokers in Australia, Canada, England and the United States, and found that cigarette smokers with depression were more motivated to quit smoking but were more likely to relapse than cigarette smokers without depression.9 Although cigarette smokers with depression may have been more motivated to quit, Cooper and colleagues discussed several reasons why they may be more likely to relapse than their counterparts without depression, including neurochemical processes that reinforce smoking, low self-efficacy, a lack of adaptive coping strategies, negative cognitive style and issues with emotion regulation.
Evidence also shows that depression is strongly associated with cannabis use,12–17 with regular cannabis use being twice as common among individuals with mental health illnesses. 15,18 Notably, the co-use of tobacco and cannabis is common,19–23 with a higher proportion of cigarette smokers using cannabis relative to those who do not smoke.24–26 Studies have found that the co-use of cannabis and tobacco (cigarette smoking) is associated with poorer mental health, alcohol misuse, more intensive tobacco use and lower rates of quitting (cigarette) smoking.23,26–32 At this time, although there is evidence that cigarette smokers in Canada are more likely to use cannabis than nonsmokers,5 little is known about the prevalence and frequency of cannabis use among cigarette smokers with and without depressive symptoms. As evidence suggests that people who use both tobacco and cannabis are more likely to report mental health problems, greater nicotine dependence and alcohol misuse, all of which are associated with reduced success in tobacco cessation, investigation as to whether co-consumers and cigarette-only smokers differ on these measures is warranted. This is important to assess in Canada, where the prevalence of cannabis use is high,5 particularly among people who smoke cigarettes, and where nonmedical (recreational) cannabis has been legal since 2018,33 allowing for greater access to cannabis among adults.
Therefore, we examined the prevalence of cannabis use and depressive symptoms among adults who currently smoke cigarettes and tested whether co-consumers of cannabis and tobacco were more likely to report depressive symptoms than cigarette-only smokers. We also tested whether cigarette-only smokers and co-consumers differed on cigarette dependence measures (frequency of smoking, cigarettes smoked per day, perceived addiction to cigarettes, urges to smoke cigarettes), motivation to quit smoking (plans to quit cigarette smoking, attempts to quit smoking cigarettes) and high-risk alcohol consumption by the presence or absence of depressive symptoms. We hypothesized that depressive symptoms would be more commonly reported by cigarette smokers who co-use cannabis. Additionally, we predicted that smokers with depressive symptoms may be more likely to be motivated to quit cigarette smoking, as found previously;9 however, we were uncertain whether cannabis use would moderate the effects of depression for each of the outcomes.
Methods
We analyzed data from the Canadian arm of the 2020 (Wave 3) International Tobacco Control Policy Evaluation Project Four Country Smoking and Vaping (ITC 4CV3) Survey, an online cohort survey designed to evaluate the psychosocial and behavioural impact of tobacco control policies on adult smokers (age ≥ 18 yr) in Australia, Canada, England and the US.34–37 The ITC 4CV3 Canada Survey included nationally representative samples of cigarette smokers, former cigarette smokers and e-cigarette users from all 10 provinces.37 Data were collected from Feb. 24 to May 31, 2020.
Nonmedical cannabis in Canada
In Canada, cannabis is legal for adult use for both medical and nonmedical purposes. Medicinal use of cannabis was legalized nationwide in July 2001. The federal Cannabis Act33 came into effect on Oct. 17, 2018, and made Canada the second country in the world, after Uruguay, to formally legalize the cultivation, possession, acquisition and consumption of nonmedical cannabis and its by-products. Cannabis legalization comes with regulation similar to that of alcohol in Canada, limiting home production, distribution, consumption areas and sale times.38 By 2019, government online sales were well underway, and licensed retail stores were being opened, making legal cannabis products more widely available to adults.
Study design and sample recruitment
Full details about the study design and sampling are provided in Appendix 1 (available at www.cmajopen.ca/content/11/3/E516/suppl/DC1). Reporting of our findings was guided by the Checklist for Reporting Results of Internet E-Surveys checklist. In brief, to be eligible for recruitment into the ITC 4CV Survey, potential respondents must be aged 18 years or older and meet 1 of the following criteria: current cigarette smoker (smokes at least monthly and has smoked at least 100 cigarettes in their lifetime); recent former smoker (has stopped smoking cigarettes in the past 24 months and has smoked at least 100 cigarettes in their lifetime); or current use of e-cigarette or heated tobacco products (currently vape nicotine or use heated tobacco products daily or weekly, irrespective of cigarette smoking). Respondents were excluded if they did not meet the above criteria, if they provided poor-quality data or if someone other than the intended person completed the survey.
The current study used cross-sectional data from the ITC 4CV3 (2020) Survey. Canadian respondents were recruited from Leger Opinion’s online probability-based panel,39 which is nationally representative of the Canadian population across age, sex, geographic region and socioeconomic status. For the ITC 4CV3 Survey, Leger Opinion identified panellists who met the inclusion criteria and invited them to be screened for the online survey. All panellists who submitted a valid survey at Wave 2 (2018) were eligible for Wave 3. Wave 2 respondents lost to follow-up were replaced by newly sampled panellists who met predetermined recruitment criteria (age ≥ 18 yr), sex, age and region criteria, and who consented to participate in the survey. Eligible panellists were provided a link to the online survey by Leger Opinion, which was hosted by the University of Waterloo Survey Research Centre. The survey questionnaire was developed by ITC investigators in collaboration with the project management and survey management teams. Leger Opinion was responsible for the recruitment and recontact of participants (e.g., invitations, reminders, monitoring of survey activity, providing remuneration, gathering of demographic information and maintaining data files). See Appendix 1 for the detailed responsibilities of Leger Opinion. The ITC survey project team was responsible for the survey fieldwork process and data management. Remuneration for participation was Can$25 for recontact respondents and $28 for replenishment respondents.
Eligibility for the current study
Based on common criteria used in tobacco and nicotine research,40–45 “current” cigarette smokers were defined as those who smoked at least 100 cigarettes during their lifetime and currently smoked at least monthly.
Data weighting and sample representativeness
Sampling weights (interpreted as the inverse probabilities of selection for the corresponding respondents) allow sample observations from a complex survey to be inflated to yield accurate population totals for population strata and key categories of interest,46 including tobacco user groups. Sampling weights adjust for the oversampling of some subpopulations, nonresponse and other sources of bias. The ITC 4CV3 study had a complex survey design that involved stratification and unequal probabilities of selection. The weights for 4CV3 were designed to make the sample as representative as possible of the adult smoker population in Canada with respect to sex, age group, educational attainment and geography. The 2019 Canadian Tobacco and Nicotine Survey42 was used as the benchmark to compute weights for the Canadian 4CV3 data. A raking algorithm46 was used to calibrate cross-sectional sampling weights on smoking status, geographic region and demographic measures (e.g., sex, age, ethnicity and education). Further information on data-weighting procedures can be found elsewhere.36,37 The full ITC 4CV3 technical report can be found in Appendix 2, available at www.cmajopen.ca/content/11/3/E516/suppl/DC1.
Measures
The ITC 4CV3 Survey is available at https://itcproject.org/surveys/canada/4cv3-ca/ and in Appendix 3, available at www.cmajopen.ca/content/11/3/E516/suppl/DC1.
Independent variables
Cannabis use
Measures from the ITC 4CV3 Survey that were used to assess cannabis use are presented in Box 1. As per the Canadian Cannabis Survey, “cannabis use” refers to using cannabis in its dry form or when mixed or processed into another product, such as an edible, a concentrate (including hashish) or a liquid. 13 Most Canadian cigarette smokers in our study who used cannabis in the last year reported smoking it (81%).
Cannabis survey questions from the International Tobacco Control Policy Evaluation Project Four Country Smoking and Vaping Survey Wave 3 used in this study
Cannabis use was determined by the following questions:
Ask all respondents: When was the last time you used marijuana/cannabis?
Never used
In the last 30 days
In the last 1–12 months
More than 1 year ago
Don’t know
Declined to answer
Among respondents who reported that they used cannabis in the last year, a subsequent question was asked to determine their frequency of use:
On average, how often do you CURRENTLY use any form of marijuana/cannabis?
Daily
Not daily, but at least weekly
Not weekly, but at least monthly
Not monthly, but occasionally
Don’t know
Declined to answer
“Current co-use” of cannabis combined above 2 questions:
Current cannabis use: used in the last 12 months, and at least monthly
No current cannabis use: never used cannabis, have not used cannabis in the last year, use cannabis occasionally (less than monthly)
Depressive symptoms
All respondents were screened for past-30-day depressive symptoms using the 2-question case-finding instrument (TQI) for depression.47 The validity of the TQI was tested by Whooley and colleagues.47 The authors reported that the TQI is a useful measure for detecting depression in primary care and has similar test characteristics to other case-finding instruments, including the Center for Epidemiologic Studies Depression Scale and Beck Depression Inventory, with high sensitivities and specificities. Whereas the TQI provides an assessment of depressive symptoms in the past 30 days, the Diagnostic and Statistical Manual of Mental Disorders states that the essential feature of a major depressive episode is a period of at least 2 weeks during which there is either depressed mood or the loss of interest or pleasure in nearly all activities. 48 Thus, the TQI likely serves as a reasonable cut-off for the presence versus absence of depressive symptoms.
The TQI includes the following 2 questions: “During the last 30 days, have you often been bothered by little interest or pleasure in doing things?” and “During the last 30 days, have you often been bothered by feeling down, depressed, or hopeless?” Respondents who reported “yes” to both questions were classified as screening positive for depressive symptoms.
Covariates
Sociodemographic characteristics
Sociodemographic data were collected by Leger Opinion and verified by the respondents at the time of survey completion, including age, sex, ethnicity, income and education.
Outcome measures
Cigarette smoking–related outcomes
Cigarette/nicotine dependence: Respondents reported their cigarette smoking frequency (daily v. nondaily), the number of cigarettes that they smoked on average (converted into cigarettes smoked per day, 0–10 v. ≥ 11), whether they perceived themselves as being very addicted to cigarettes (v. not at all/somewhat/don’t know), and whether they had strong/very/extremely strong urges to smoke in the last 24 hours (v. none/slight/moderate/don’t know).
Motivation to quit smoking: Respondents reported whether they had made an attempt to quit smoking cigarettes in the last 24 months ([a] at least once v. none/don’t know; [b] made multiple quit attempts [≥ 2] v. one/none/don’t know), and whether they planned to quit smoking in the next 6 months (v. not planning to quit within 6 months/not planning to quit at all/don’t know).
Alcohol use
Risky alcohol consumption, adapted from the National Institute on Alcohol Abuse and Alcoholism’s definition of drinking levels,49 was defined as “low-risk” drinking (≤ 4 drinks per occasion for men, ≤ 2 drinks per occasion for women) and “high-risk” drinking (≥ 5 drinks per occasion for men, ≥ 3 drinks per occasion for women, and ≥ 6 drinks on a single occasion at least once a month for men and women). The comparison group was infrequent drinking or abstains from drinking, where infrequent drinking was defined as drinking only once per month or less often and never consuming more than 6 drinks on those occasions.
Statistical analysis
Unweighted descriptive statistics were used to describe the study sample of adult cigarette smokers in Canada, overall and by depressive symptoms. Weighted descriptive statistics were used to estimate the prevalence of depressive symptoms, overall and by cannabis use status, and to test whether depressive symptoms were more commonly reported by co-consumers than by cigarette-only smokers.
Weighted multivariable logistic regression models were used to test whether cigarette smoking–related outcomes and high-risk alcohol consumption differed between co-consumers and cigarette-only smokers, stratified by depressive symptoms (presence v. absence). We also reported the main effects for depression and cannabis use for each outcome and tested whether there was an interaction between cannabis use and depressive symptoms. All models were adjusted for age (18–39 v. ≥ 40 yr), sex (male v. female), education (low, moderate, high, not reported) and income (low, moderate, high, not reported). Frequency of cigarette smoking was also used as a covariate in all models, except for daily smoking and cigarettes smoked per day. All analyses were conducted using the survey procedures in SAS version 9.4.
Ethics approval
The ITC 4CV Canada Survey protocols and all materials, including the survey questionnaires, were approved by the Office of Research Ethics at the University of Waterloo (REB#20803/30570). All participants provided consent to participate.
Results
The retention rate for Wave 3 Canadian cohort respondents (those retained between Waves 2 and 3) was 43.9%. The response rate for the newly recruited participants was 14.6%, with a cooperation rate (percentage of eligible respondents who completed the survey) of 93.2%.
Study sample
A total of 3688 Canadian respondents completed the 2020 survey; 2843 were current smokers (smoked at least monthly). Those who smoked less than monthly (n = 71), formerly (n = 618) and never smoked (n = 156) were excluded from this study. Appendix 4 (available at www.cmajopen.ca/content/11/3/E516/suppl/DC1) presents the study selection process. The median time for survey completion among Canadian respondents was 48.6 minutes.
Demographic, cigarette smoking and cannabis use characteristics of the study sample are presented in Table 1.
Demographic and smoking and cannabis use characteristics of the study sample, unweighted*
Self-reported depressive symptoms among cigarette smokers, overall and by cannabis co-use status
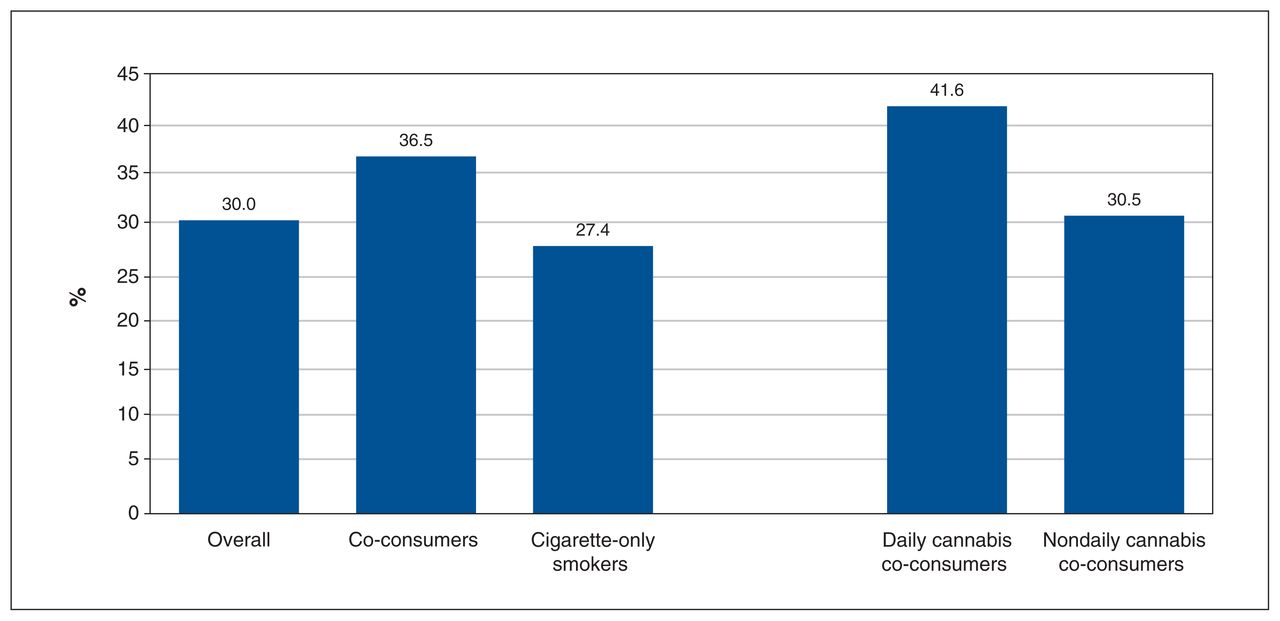
Figure 1 shows self-reported depressive symptoms among cigarettes smokers in Canada, overall and by cannabis use status. Overall, 30.0% of survey respondents reported depressive symptoms. Respondents who reported current cannabis use (co-consumers) were more likely to report depressive symptoms (36.5%) than those who did not report current cannabis use (27.4%; adjusted odds ratio [OR] 1.5, 95% confidence interval [CI] 1.2–1.9). Co-consumers who used cannabis daily had a significantly higher rate of depressive symptoms (41.6%) than nondaily cannabis co-consumers (30.5%, adjusted OR 1.63, 95% CI 1.16–2.29) and cigarette-only smokers (adjusted OR 1.91, 95% CI 1.48–2.47).

Self-reported (past-30-day) depressive symptoms among cigarette smokers in Canada, overall and by cannabis co-use status. Data are weighted and unadjusted for age, sex, education, income and cigarette smoking frequency. Cigarette smokers who reported current cannabis use were more likely to report depressive symptoms than those who did not report current cannabis use (adjusted OR 1.5, 95% CI 1.2–1.9). Co-consumers who used cannabis daily had a significantly higher rate of depressive symptoms than nondaily cannabis co-consumers (adjusted OR 1.6, 95% CI 1.2–2.3) and cigarette-only smokers (adjusted OR 1.9, 95% CI 1.5–2.5). Note: CI = confidence interval, OR = odds ratio.
Prevalence of cannabis use among current cigarette smokers, overall and by self-reported depressive symptoms
Among all respondents, 59 did not report valid information for cannabis use in the last year (declined to answer, n = 19; or did not know, n = 40) and were marked as missing in the analysis. As shown in Table 2, the prevalence of past-year and past-30-day cannabis use was 44.0% and 33.2%, respectively; 30.4% reported using cannabis at least monthly, and 16.1% daily. Survey respondents with depressive symptoms were significantly more likely to report past-year cannabis use, past-30-day use, at least monthly cannabis use and daily cannabis use than those without depressive symptoms (all p < 0.001).
Weighted descriptive estimates of prevalence of cannabis use among adult current cigarette smokers in Canada, overall and by self-reported past-30-day depressive symptoms*
Comparison of cigarette smoking–related variables and alcohol use between co-consumers and cigarette-only smokers by depressive symptom status
As shown in Table 3, respondents with depressive symptoms (co-consumers and cigarette-only smokers) had higher rates of perceiving themselves as being very addicted to cigarettes, reported having strong urges to smoke and had made an attempt to quit smoking in the last 24 months (as well as multiple attempts to quit), whereas co-consumers and cigarette-only smokers without depressive symptoms were similar on most measures (there were no significant differences between these 2 groups).
Multivariable regression models comparing cigarette smoking–related variables and alcohol use between cigarette-only smokers and cigarette smokers who co-use cannabis, by presence versus absence of depressive symptoms*
When we examined the independent effects of cannabis use and depressive symptoms, depressive symptoms were associated with planning to quit smoking (p = 0.01), having made an attempt or multiple attempts to quit smoking (p < 0.001), the perception of being very addicted to cigarettes (p < 0.001) and strong urges to smoke (p = 0.001), whereas cannabis use was not (all p ≥ 0.05). With regard to alcohol use, cannabis use was associated with high-risk alcohol consumption (p < 0.001), whereas depressive symptoms were not (p = 0.1). Notably, co-consumers with depressive symptoms reported the highest rate of high-risk alcohol use (35.0%), followed by co-consumers without depressive symptoms (29.3%), and cigarette-only smokers with (20.0%) and without depressive symptoms (15.3%). There were no interaction effects between current cannabis use and depressive symptoms on any of the outcome measures, suggesting cannabis use and depression did not influence the magnitude or direction of the effect of the other. Appendix 5 (available at www.cmajopen.ca/content/11/3/E516/suppl/DC1) presents the adjusted ORs and 95% CIs for the independent (main) effects of depressive symptoms and cannabis use on cigarette smoking–related variables and alcohol use.
Interpretation
This study fills several gaps in the literature by examining the prevalence of cannabis use and depressive symptoms in a sample of cigarette smokers in Canada. Overall, 44% of our sample of current smokers reported using cannabis in the previous year, 33% reported using cannabis in the past 30 days and 16% reported using cannabis daily. In 2020, the Canadian Cannabis Survey found that 27% of Canadian adults used cannabis in the last 12 months, with provincial and territorial estimates ranging from 21% to 37%.13 Thus, the current study shows that our sample of adults who smoke cigarettes report using cannabis at a higher average rate than the general adult population, which is consistent with other studies in the US,25 the United Kingdom26 and Canada.24,50
The percentage of participants who screened positive for depressive symptoms in our sample was 30%, which is higher than the rate of Canadians who report mental illness,51 including depression, in the general population.52 Studies have shown that adults who smoke cigarettes have higher levels of depression than people who do not smoke.6 We found that a higher percentage of respondents using cannabis reported depressive symptoms (37%) than respondents who were not currently using cannabis (28%). This corroborates evidence that adults who use cannabis have higher rates of depression than those who do not use cannabis.12,15,16 Notably, studies have shown that individuals with depression are at increasing risk of cannabis use, with a particularly strong increase in daily or near-daily cannabis use.12,53 Additionally, cigarette smokers who were using cannabis daily reported a higher rate of depressive symptoms (42%) than those who were using cannabis nondaily (31%) or not using cannabis at all (27%). Thus, our findings are consistent with those of other studies that have reported co-use of cannabis and tobacco to be associated with poorer mental health, particularly among those who use cannabis more frequently.26,27,54
Our study results showed associations that have implications for clinical practice. First, cigarette-only smokers and co-consumers without depressive symptoms did not differ on any of the cigarette-dependence measures or motivation to quit smoking. In contrast, co-consumers and cigarette-only smokers with depressive symptoms were more likely to perceive themselves as more addicted to cigarettes and had stronger urges to smoke than respondents without depressive symptoms but, interestingly, did not differ on their self-reported cigarette consumption. Previous studies have found that co-consumers have greater nicotine dependence,20,26,54,55 and our findings are not consistent with this, as we found that several cigarette smoking–related variables were associated with depression, but not cannabis use. This requires further investigation using carefully designed studies that can disentangle the nature and direction of these effects. However, our results suggest that clinicians and providers should consider screening for depression among cigarette smokers and address perceived addiction with behavioural counselling to help patients move toward successful smoking cessation, while addressing both depressive symptoms and tobacco dependence.
Our findings support previous evidence that smokers with depression are more motivated to quit smoking than their counterparts without depression (e.g., made multiple attempts to quit smoking).8–11 We found that depression was associated with making at least 1 attempt to quit smoking in the last 24 months, as well as having made multiple attempts to quit, but cannabis use was not. Thus, smoking cessation treatment should focus not only on the quit attempt, but also on how to keep smokers who are experiencing depression from relapsing.
High-risk alcohol consumption has been found to be a barrier to making an attempt to quit cigarette smoking, and successful smoking cessation, particularly among those with substance use disorders.56,57 We found that cannabis use was associated with high-risk alcohol consumption among our sample of adult cigarette smokers, whereas depressive symptoms were not. However, co-consumers with depressive symptoms had the highest rate of alcohol misuse. Thus, our findings, as well as those of other studies, suggest that smoking cessation should be integrated into the routine care of patients who consume alcohol and other drugs.58,59
Limitations
Although this was a large study relying on a representative sample of current smokers in Canada, there are some limitations to consider. Because this was a cross-sectional study, the directional relation between depression, cannabis use and cigarette smoking cannot be determined with the outcomes measured. The sample was limited to adults in Canada who smoked cigarettes at least monthly, so observations may not apply to other populations of interest, including youth, adults who smoke less than monthly, or cigarette smokers in other countries. This study was conducted during the early phase of the COVID-19 pandemic, and as a result, these findings may differ from those in prepandemic or later pandemic periods. However, studies in Canada generally found no net changes in cannabis or cigarette consumption in early 2020,13,60,61 so we would not expect large differences based on the timing of this survey. The TQI measure used in this study to determine the presence of depressive symptoms is limited in detecting a history of depression or depressive severity. People with a longer or more severe history of depression may differ significantly from those who have more recent or mild depressive symptoms. Although the weights for 4CV3 data were designed to make the sample as representative as possible of the adult smoker population in Canada, the decision to participate is likely to depend on some unmeasured characteristics that may be associated with outcomes or relationships of interest. For example, although we weight for educational attainment, a major influence on response propensity, we recognize that there may be additional ways in which even the weighted sample may have limited representativeness. Finally, the measures used in this study were based on self-report and therefore may be subject to recall bias.
Conclusion
In a survey of adults in Canada who smoke cigarettes, about one-third reported current cannabis use. Depressive symptoms were more common among those who were co-using cigarettes and cannabis. Several cigarette smoking–related variables were associated with depression, but not cannabis use, whereas cannabis use was strongly associated with alcohol misuse. Tobacco cessation treatment may require multi-pronged strategies to address mental health, alcohol misuse or cannabis use — co-factors that may reduce cigarette cessation activity.
Footnotes
Competing interests: Geoffrey Fong has served as an expert witness or consultant on behalf of governments defending their country’s policies or regulations in litigation. Geoffrey Fong and Shannon Gravely served as paid expert consultants to the Ministry of Health of Singapore in reviewing the evidence on plain and standardized packaging. Geoffrey Fong was a member of the Health Canada Vaping Products Scientific Advisory Group (2017–2020; unpaid). No other competing interests were declared.
This article has been peer reviewed.
Contributors: Shannon Gravely, Pete Driezen, Erin McClure, Danielle Smith and Geoffrey Fong contributed to the conceptualization, investigation and interpretation of data. Geoffrey Fong contributed to funding acquisition. All authors revised the manuscript for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This International Tobacco Control Policy Evaluation Project (ITC) Four Country Smoking and Vaping Survey study was supported by grants from the US National Cancer Institute (P01 CA200512), the Canadian Institutes of Health Research (FDN-148477) and the National Health and Medical Research Council of Australia (APP 1106451). Geoffrey Fong was supported by a Senior Investigator Award from the Ontario Institute for Cancer Research (IA-004). The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. The sponsors had no role in the design, data collection, data analysis, data interpretation or writing of the report. All inferences, opinions and conclusions drawn in this manuscript are those of the authors, and do not reflect the opinions or policies of the data stewards.
Data sharing: In each country participating in the ITC Project, the data are jointly owned by the lead researcher(s) in that country and the ITC Project at the University of Waterloo. Data from the ITC Project are available to approved researchers 2 years after the date of issuance of cleaned data sets by the ITC Data Management Centre. Researchers interested in using ITC data are required to apply for approval by submitting an International Tobacco Control Data Repository (ITCDR) request application and subsequently to sign an ITCDR Data Usage Agreement. The criteria for data usage approval and the contents of the Data Usage Agreement are described online (http://www.itcproject.org).
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/3/E516/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.