


Article Figures & Tables
Figures
- Figure 1:
Flow chart of cohort creation. The cohorts consist of users of the originator infliximab. Gastrointestinal (GI) conditions included ulcerative colitis and Crohn disease. Low compliance or infliximab discontinuation was defined as no medication supply on May 27 combined with no refill in the 84 days before (excluding) May 27. Switching was defined as a refill of a different biologic anti-inflammatory medication or the biosimilar version of infliximab. Short follow-up was defined as less than 1 month of medical plan enrolment starting on the cohort entry date (May 27). PharmaCare coverage was determined based on all originator infliximab refills during the 6-month period before May 27. *The number of patients who switched was less than 6. †The number of patients with follow-up duration shorter than 1 month was less than 6.
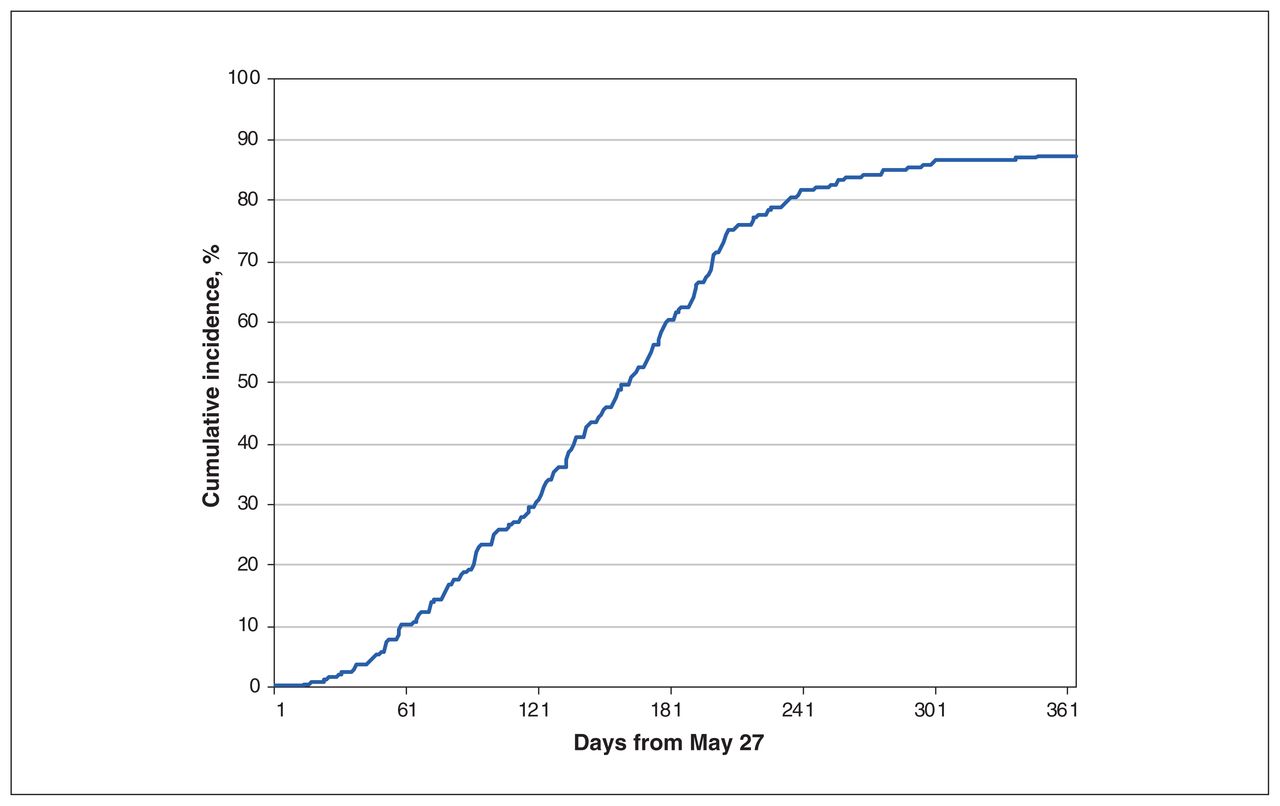
- Figure 2:
Cumulative incidence of switching to the biosimilar infliximab, policy cohort (n = 377).
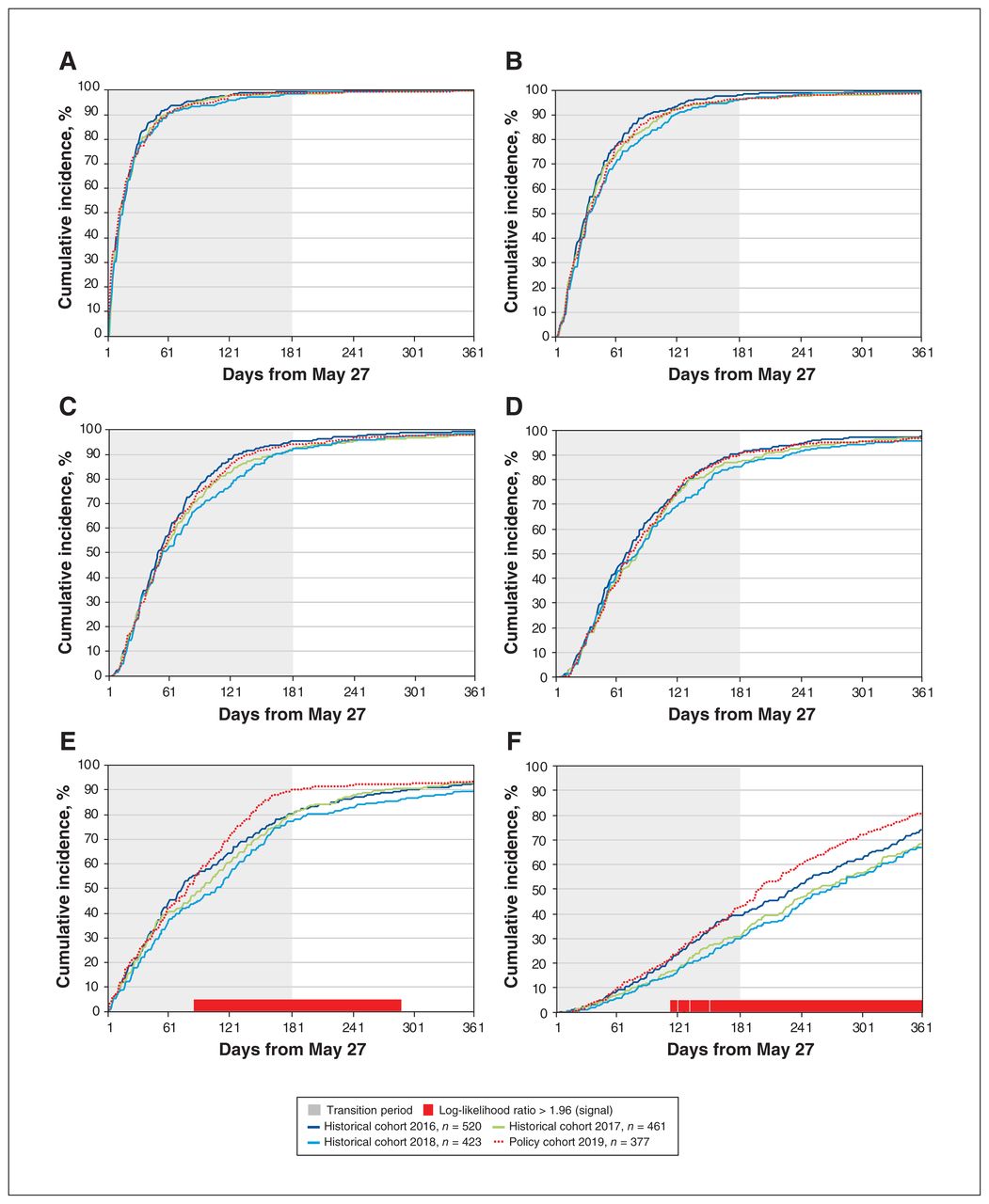
- Figure 3:
Cumulative incidence of filling the first (A), second (B), third (C) and fourth (D) prescriptions of infliximab and switching to a different biologic or targeted synthetic disease-modifying antirheumatic drug (E) during the 1-year follow-up period, by cohort. Cumulative incidence is expressed as the percentage of patients in each cohort who experienced the outcome by day of follow-up. The 6-month transition period of the policy is shaded in grey. Days with log-likelihood ratios comparing the policy cohort and the average of the historical cohorts above the threshold of 1.96 are marked by a red block.
- Figure 4:
Cumulative incidence of the first (A), second (B), third (C) and fourth (D) visits to a physician and the first (E) and second (F) visits to a specialist during the 1-year follow-up period, by cohort. Cumulative incidence is expressed as the percentage of patients in each cohort who experienced the outcome by day of follow-up. The 6-month transition period of the policy is shaded in grey. Days with log-likelihood ratios comparing the policy cohort and the average of the historical cohorts above the threshold of 1.96 are marked by a red block.
- Figure 5:
Cumulative incidence of the first visit to an emergency department (A) and the first discharge from hospital (B) during the 1-year follow-up period, by cohort. Cumulative incidence is expressed as the percentage of patients in each cohort who experienced the outcome by day of follow-up. The 6-month transition period of the policy is shaded in grey. Hospital data were available until Mar. 26, 2020.





Tables
Characteristic Infliximab cohort; no. (%) of patients* Historical cohort 2016
n = 520Historical cohort 2017
n = 461Historical cohort 2018
n = 423Policy cohort 2019
n = 377Age, yr Mean ± SD 56.4 ± 15.7 57.4 ± 16.0 58.3 ± 15.6 58.6 ± 15.7 Median (range) 57.5 (6.0–91.0) 58.0 (4.0–90.0) 59.0 (7.0–91.0) 60.0 (8.0–91.0) Sex Female 289 (55.6) 247 (53.6) 228 (53.9) 200 (53.1) Male 231 (44.4) 214 (46.4) 195 (46.1) 177 (46.9) Most likely diagnosis Any rheumatologic diagnosis 480 (92.3) 422 (91.5) 387 (91.5) 345 (91.5) Rheumatoid arthritis 278 (53.5) 242 (52.5) 218 (51.5) 190 (50.4) Ankylosing spondylosis 115 (22.1) 109 (23.6) 101 (23.9) 90 (23.9) Psoriatic arthritis 45 (8.7) 41 (8.9) 38 (9.0) 30 (8.0) Psoriasis 19 (3.7) 15 (3.3) 17 (4.0) 15 (4.0) Undetermined 21 (4.0) 24 (5.2) 19 (4.5) 17 (4.5) Time from first infliximab use, yr, mean ± SD 7.2 ± 4.5 8.5 ± 4.4 9.6 ± 4.3 10.6 ± 4.3 Health services utilization in previous year, mean ± SD No. of different medications Any medication† 9.3 ± 6.0 9.3 ± 6.2 8.7 ± 5.4 8.7 ± 5.6 Biologic anti-inflammatory medications‡ 1.1 ± 0.3 1.0 ± 0.1 1.0 ± 0.0 1.0 ± 0.0 Conventional synthetic anti-inflammatory medications§ 0.8 ± 0.8 0.8 ± 0.8 0.8 ± 0.8 0.7 ± 0.7 No. of visits to physicians¶ 23.2 ± 16.7 23.1 ± 17.9 21.7 ± 14.6 20.9 ± 15.0 No. of nights in hospital** 1.0 ± 5.2 0.8 ± 3.9 0.6 ± 3.6 0.5 ± 2.6 SD = standard deviation.
↵* Except where indicated otherwise.
↵† Based on non-brand names of prescription medications.
↵‡ Biologic anti-inflammatory medications were adalimumab, etanercept, certolizumab, golimumab, abatacept, tocilizumab, anakinra, tofacitinib, rituximab, ustekinumab, secukinumab, ixekizumab, brodalumab and guselkumab.
↵§ Conventional synthetic anti-inflammatory medications were methotrexate, hydroxychloroquine, leflunomide, sulfasalazine, minocycline, azathioprine, auranofin, chloroquine, cyclophosphamide, cyclosporine, gold sodium thiomalate, mycophenolate and penicillamine.
↵¶ Visits to physician of any specialty, in an outpatient setting, are included, regardless of whether the subsequent visit was to the same physician.
↵** Includes all nights in hospital, regardless of whether the admission was associated with an emergency department visit.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.