


Abstract
Background: Endovascular thrombectomy (EVT) has revolutionized ischemic stroke care. We aimed to assess whether neighbourhood socioeconomic status is predictive of access to EVT after receipt of alteplase for ischemic stroke among patients living in Alberta, Canada, and whether this relation is mediated by the distance a person lives to the nearest comprehensive stroke centre (CSC).
Methods: We performed a retrospective study including all people older than 18 years living in Alberta who were admitted to hospital with an ischemic stroke and who received intravenous alteplase treatment between Jan. 1, 2017, and Dec. 31, 2019. Data were obtained through administrative data sets. The primary outcome was treatment with EVT. We assigned neighbourhood deprivation quintile based on the Material and Social Deprivation Index. We used logistic regression modelling to assess for a relation between deprivation and treatment with EVT. We adjusted for age, sex, stroke severity and distance to the nearest CSC. We calculated the average causal mediation effect of distance to the nearest CSC on the relation between neighbourhood deprivation level and treatment with EVT.
Results: The study cohort consisted of 1335 patients, of whom 181 (13.6%) had missing data and were excluded from the main regression analysis. Endovascular thrombectomy was performed or attempted in 314 patients (23.5%). In the primary model, patients from the most deprived neighbourhoods were less likely than those from less deprived neighbourhoods to have received EVT (adjusted odds ratio 0.43, 95% confidence interval 0.24 to 0.77). Neighbourhood deprivation level was not significantly associated with EVT when distance to the nearest CSC was included as a covariate. Mediation analysis suggested that 48% of the total effect that neighbourhood deprivation level had on the odds of receiving EVT was attributable to the distance a person lived from the nearest CSC.
Interpretation: The results suggest that people from more deprived neighbourhoods in Alberta were less likely to be treated with EVT than those from less deprived neighbourhoods. Improving access to EVT for people living in remote locations may improve the equitable distribution of this treatment.
Acute ischemic stroke is the most common form of cerebrovascular disease and typically results from the sudden occlusion of a cerebral artery.1 Ischemic stroke remains a leading cause of morbidity and mortality worldwide.2 Early treatment goals are centred around reperfusing the affected brain, which traditionally has been accomplished by intravenous administration of thrombolytic medications within 4.5 hours of stroke onset.3 More recently, endovascular thrombectomy (EVT) has revolutionized the treatment of ischemic stroke. Multiple randomized controlled trials have shown that EVT together with intravenous thrombolytic therapy was superior to intravenous thrombolytic therapy alone in preventing death and disability after ischemic stroke.4–10 It has since been considered standard of care at the comprehensive stroke centres (CSCs) in Alberta, Canada. Endovascular thrombectomy is best performed within 6 hours of stroke onset, as it reperfuses the ischemic brain and prevents further progression of cell death.11,12 This treatment is resource intensive and is available only at CSCs. Several studies using the US National Inpatient Sample database showed an association between geographic markers of socioeconomic status and the odds of being treated with EVT.13–16 However, to our knowledge, this association has not been investigated in the context of Canada’s health care system. Unlike the United States, Canada has a publicly funded health care system that ensures Canadians access to medically necessary hospital and physician services without paying out of pocket, which eliminates a financial barrier to accessing health care.
The objective of this work was to assess whether neighbourhood socioeconomic status is predictive of access to EVT after receipt of alteplase for ischemic stroke among patients living in Alberta. A secondary aim was to assess whether any discrepancy in the odds of receiving EVT is mediated by the distance a person lives from the nearest CSC.
Methods
Setting
This study was performed in Alberta, which has a population of more than 4 million people.17 Endovascular thrombectomy is performed only at the 2 CSCs: the University of Alberta Hospital, in Edmonton, and Foothills Medical Centre, in Calgary. The province has a single public health care provider, Alberta Health Services.
Data and population
We performed a retrospective analysis of the Quality Improvement & Clinical Research database, a prospective data set established in 2015 that is maintained by the Cardiovascular and Stroke Strategic Clinical Network at Alberta Health Services.18 The database includes information for all patients treated with intravenous thrombolysis or endovascular thrombectomy, or both, for ischemic stroke in Alberta. We included all people older than 18 years living in Alberta who were admitted to hospital with an ischemic stroke and who received intravenous alteplase treatment between Jan. 1, 2017, and Dec. 31, 2019. Patients’ clinical and demographic characteristics were extracted from the Quality Improvement & Clinical Research database and Alberta Health Services Data and Analytics (formerly Data Integration, Measurement and Reporting) administrative databases.19 Case linkage was done through medical record numbers, which were consistent across both data sets. Database extraction and linkage were performed by one of the authors (D.B.-I.). Postal codes were obtained from the Data and Analytics database.
Independent variable of interest
In Canada, the most widely used measure of neighbourhood socioeconomic status is the Material and Social Deprivation Index, an area-based metric for assessing material and social deprivation.20,21 Scores are based on the smallest geographic unit collected in the Canadian census, the dissemination area.22 Although the Material and Social Deprivation Index was initially created for the province of Quebec alone, it has since been expanded to cover the whole of Canada and has been shown to have an association with death after stroke.23,24
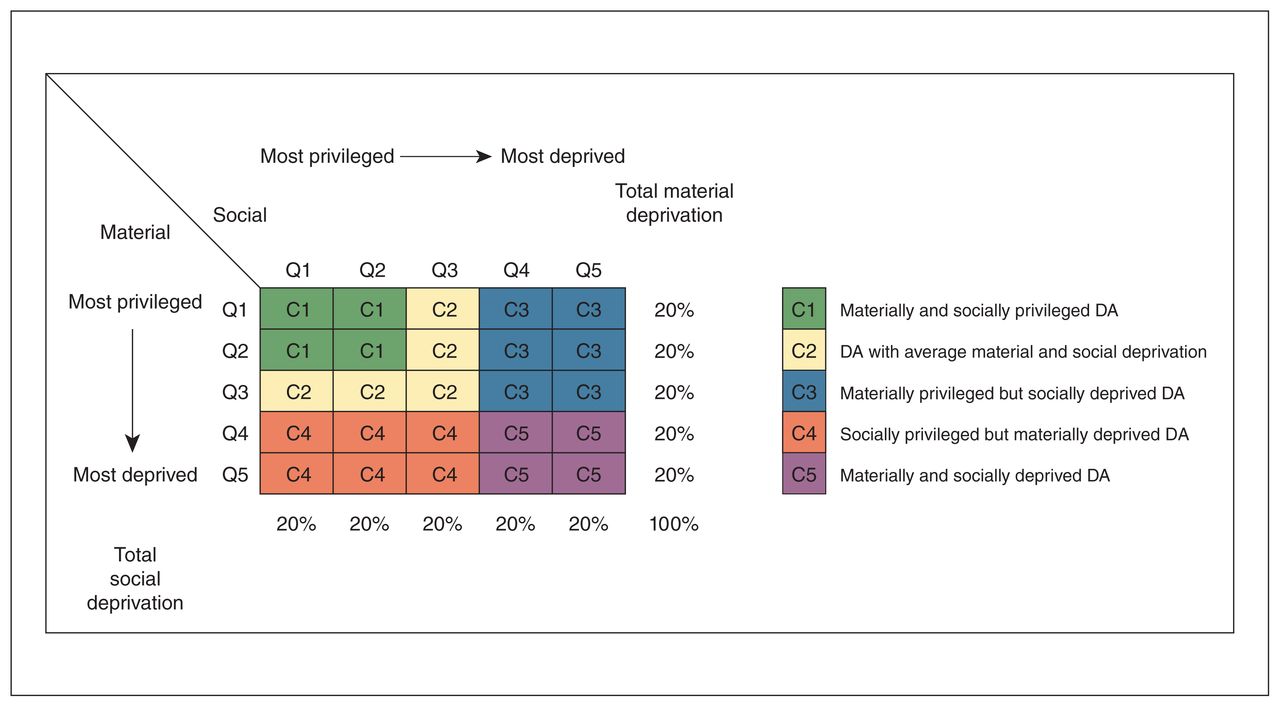
We linked patient home address postal codes to the federal census dissemination areas in Alberta.25 We assigned a Material and Social Deprivation Index score to each dissemination area using an established deprivation index (Pampalon index)26 that has been validated for use across Canada.27 For both material and social deprivation, scores are grouped into quintiles ranging from 1 (least deprived) to 5 (most deprived). We combined material and social deprivation quintiles based on the method suggested by Gamache and colleagues26 to create an overall measure of socioeconomic deprivation for use in the statistical analyses (Figure 1).

Combination of material and social deprivation quintiles (Qs) to create a 5-group ordinal variable. Reproduced from Gamache et al.26 with permission. Note: DA = dissemination area.
Outcome of interest
The primary outcome of interest was the odds of being treated with EVT after receiving intravenous alteplase treatment for ischemic stroke. All patients in whom EVT was attempted were deemed to have been treated with EVT, regardless of whether the vessel was opened successfully with the intervention.
The total effect of neighbourhood socioeconomic status on the odds of receiving EVT can be divided into a direct effect (the effect of neighbourhood socioeconomic status on our outcome of interest) and an indirect effect (the proportion of the direct effect attributable to a third variable, in this case, distance to the nearest CSC). The indirect effect is termed the average causal mediation effect. We analyzed whether the relation between treatment with EVT and neighbourhood socioeconomic status was mediated by the distance a person lives from a CSC according to the steps outlined by Baron and Kenny.28 To isolate the mediated effect of distance on this relation, we included an abbreviated model in our mediation analysis with distance to the nearest CSC as the only covariate. The mediation model investigated the discrepancy in the odds of receiving EVT between the most and least deprived neighbourhoods in Alberta.
We examined the home address postal code for all patients in the data set to ensure they were residents of Alberta. We calculated the distance, in kilometres, from the centre of each postal code to the nearest CSC in Alberta (University of Alberta Hospital or Foothills Medical Centre) using ArcGIS Pro (Esri) for geocoding and the NAD83 / UTM zone 11 map projection (Esri). We examined the relation between distance to the nearest CSC and neighbourhood deprivation using the Kruskal–Wallis test.
Statistical analysis
We used descriptive statistics to examine the baseline characteristics of the study cohort. We assessed continuous variables for an association with the outcome of interest using the Student t test and categoric variables using the Pearson χ2 test. To assess the relation between our independent variables of interest and our primary outcome, we performed a χ2 test and fit 3 multiple logistic regression models. All covariates for the model were selected a priori based on clinical relevance. In the first model, we included age, sex and pre-alteplase National Institutes of Health Stroke Scale score as covariates. The National Institutes of Health Stroke Scale score is a numerical marker of stroke severity, with higher numbers indicating a more severe stroke.29 In a secondary model, we included distance to the nearest CSC as a covariate. We also included age and distance to the nearest CSC as potential effect modifiers using interaction terms and tested them for significant effect modification using the Wald test. Last, we performed a formal mediation analysis using the mediate function of the R package mediation (R Foundation for Statistical Computing).30 We calculated the average causal mediation effect of distance to the nearest CSC on the odds of being treated with EVT between people from the most deprived and least deprived neighbourhoods in Alberta. The mediation analysis was based on our logistic regression models. The mediation package requires prespecified investigational and control groups. Because people from the most deprived neighbourhoods had the lowest proportion of patients treated with EVT, they were considered the investigational group. Those from the least deprived neighbourhoods were designated the control group. We used a bootstrapping method with 500 simulations. We performed all modelling using a complete case analysis; however, to ensure there was no selection bias in treatment with EVT for people for whom deprivation quintile was missing, we performed a sensitivity analysis that included people with missing data as a separate group.
Statistical significance was set at p = 0.05. We performed all statistical analyses using R (R Foundation for Statistical Computing).
Ethics approval
This study received ethics approval from the University of Calgary Conjoint Health Research Ethics Board.
Results
A total of 1400 people experienced an ischemic stroke and received intravenous alteplase treatment in Alberta between Jan. 1, 2017, and Dec. 31, 2019. Of the 1400, 65 were not residents of Alberta and were excluded from the analysis, leaving 1335 patients, of whom 181 (13.6%) had missing data and were excluded from the main regression analysis. Endovascular thrombectomy was attempted in 314 (23.5%) of the 1335 patients; the proportions for quintiles 1, 2, 3, 4 and 5 were 26.8%, 24.7%, 26.3%, 25.0% and 16.2%, respectively. The baseline and clinical characteristics of the study cohort are presented in Table 1.
Baseline and clinical characteristics of the study cohort
Distance to nearest comprehensive stroke centre and deprivation level
The median distance to the nearest CSC was significantly greater for patients from the most deprived neighbourhoods than for those from the least deprived neighbourhoods (74.1 km [interquartile range 166.0 km] v. 17.4 km [interquartile range 23.4 km]) (p = 0.002) (Figure 2).

Box plot showing relation between socioeconomic deprivation level and log-transformed distance to the nearest comprehensive stroke centre (CSC). Distance log was transformed for graphical purposes to better illustrate differences. Level 1 = least deprived, level 5 = most deprived.
Endovascular thrombectomy and deprivation level
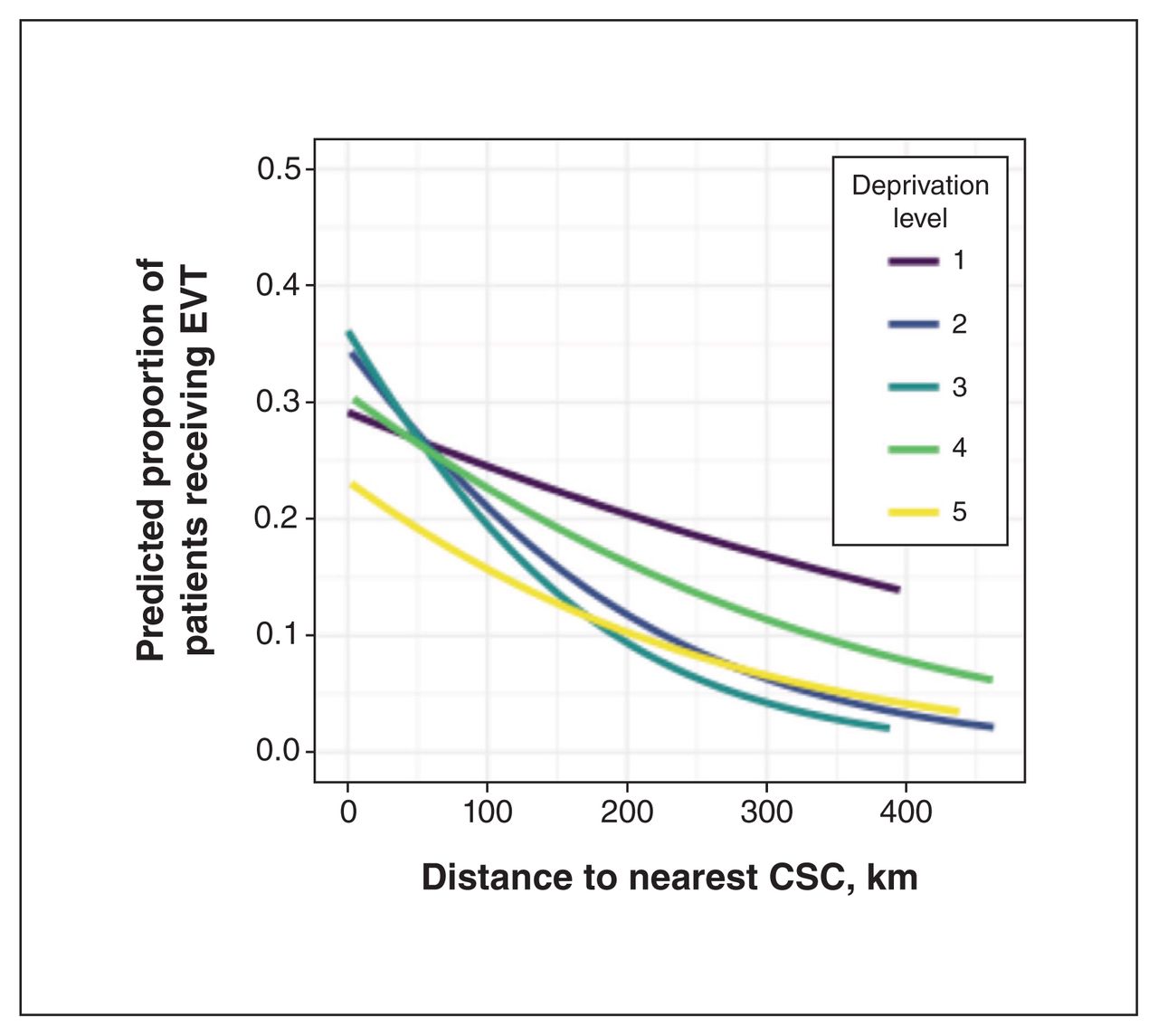
Bivariate logistic regression showed a statistically significant relation between being in the most deprived quintile and being treated with EVT (p = 0.04) (Table 2). The unadjusted odds ratio (OR) for patients from the most deprived compared to the least deprived areas was 0.53 (95% confidence interval [CI] 0.32 to 0.87). We did not observe any evidence of significant effect modification (p > 0.05). As such, the regression models did not contain any interaction terms. In the primary logistic regression model, patients from the most deprived neighbourhoods were significantly less likely to be treated with EVT than those from the least deprived neighbourhoods (OR 0.43, 95% CI 0.24 to 0.77) (Table 2). The predicted proportion of patients who would receive EVT decreased with increasing distance to the nearest CSC, regardless of neighbourhood deprivation quintile (Figure 3). In the secondary model, neighbourhood deprivation quintile was not significantly associated with the odds of receiving EVT, although there was a significant inverse relation between the distance to the nearest CSC and the odds of receiving EVT (Table 2).
Regression analysis of odds of being treated with endovascular thrombectomy

Logistic regression lines of best fit showing the predicted proportion of patients who would receive endovascular thrombectomy (EVT) based on the distance they lived from the nearest comprehensive stroke centre (CSC), stratified by deprivation level. Each line represents a separate within-deprivation-level logistic regression model.
Mediation analysis
The average causal mediation effect of distance to the nearest CSC on the odds of being treated with EVT, between patients from the most deprived neighbourhoods and those from the least deprived neighbourhoods, was −0.06 (95% CI −0.08 to −0.03). This represents 48% of the effect living in the most deprived neighbourhood compared to the least deprived neighbourhood had on being treated with EVT (total effect = −0.11, 95% CI −0.20 to −0.03).
Sensitivity analysis
There was no significant relation between missing deprivation quintile and the odds of receiving EVT (OR 0.79, 95% CI 0.47 to 1.33).
Interpretation
The results of our unadjusted analysis suggest that people who live in the most socioeconomically deprived areas of Alberta may be less likely to be treated with EVT after receiving alteplase for ischemic stroke than people who live in the least deprived areas of the province. However, our secondary model and mediation analysis showed that the distance a person lived from the nearest CSC accounted for much of this discrepancy. These findings suggest that health care providers are not systematically excluding patients from the most deprived neighbourhoods from this novel treatment, which is encouraging. Nonetheless, disparities may persist. The most deprived neighbourhoods tend to be farther away from CSCs than areas with lower deprivation levels. As such, it may take longer for patients from the most deprived parts of Alberta to get to an EVT-capable centre, thereby decreasing the odds they will be treated with EVT after an ischemic stroke. Ultimately, these findings highlight the challenges of ensuring equitable distribution of time-sensitive interventions to geographically isolated populations.
Before the advent of EVT, the best way of reperfusing ischemic brain during a stroke was thrombolysis with intravenously administered alteplase.3,31 This remained the standard of care until 2015, when several clinical trials that showed EVT in addition to alteplase was superior to alteplase alone for treatment of ischemic stroke due to large-vessel occlusion in the anterior circulation.4–8 However, there are limited data on whether the benefits from this treatment advance have been equitably distributed along socioeconomic lines. Two US papers published in 2014, one looking at 2006–2010 and the other looking at only 2008, used data from the National Inpatient Sample database to assess the relation between socioeconomic status and treatment with EVT.13,14 Both studies showed a statistically significant difference in the odds of being treated with EVT for patients living in areas with the lowest median income; however, both papers used data collected before EVT was considered the standard of care. More recently, de Havenon and colleagues15 and Mehta and colleagues16 also used the National Inpatient Sample database to investigate the relation between socioeconomic status and treatment with EVT; both teams found that patients with low socioeconomic status were less likely to be treated with EVT than patients with higher socioeconomic status. Neither group restricted their cohort to patients who received alteplase for their ischemic stroke. Although de Havenon and colleagues15 controlled for whether patients lived in an urban or rural area, neither group controlled for the distance a person lived to the nearest CSC.
To our knowledge, no study has investigated the relation between neighbourhood socioeconomic status and receipt of EVT after alteplase administration for ischemic stroke in Canada. We included only patients who were treated with alteplase, which was the previous standard of care. Nonetheless, our results are notable for suggesting that some of the disparity in access to acute stroke intervention between the most and least deprived areas in Alberta is explained by the fact that socioeconomically deprived people tend to live farther from CSCs than people who are less deprived.
The results of our mediation analysis suggest that the discrepancy in access to EVT based on neighbourhood deprivation level is mediated by the distance a person lives to the nearest CSC. Although provinces in Canada are responsible for providing health care to all residents, the reality is more complicated. In a recent review of Canada’s health care system, Marchildon and colleagues32 argued that, despite publicly funded health care, people living in rural and remote areas have less access to hospitals and other centres where they can access health care than those from urban and suburban areas. There is also a lower density of health care providers in rural and remote areas. This is of particular relevance for time-sensitive interventions such as EVT for ischemic stroke.11,12 A recent US study suggested that people living in rural areas are less likely than those from urban areas to be brought to an EVT-capable centre after an ischemic stroke, and this significantly decreases the odds that they will receive treatment with EVT, regardless of the facility’s transfer capability.33 It is not surprising that people who live far from CSCs in Alberta are also less likely to receive EVT than people who live closer to such centres, given that EVT is a time-sensitive intervention. We found that patients from the most deprived neighbourhoods were significantly more likely to live farther from the nearest CSC than patients from less deprived areas. As such, it appears that the relation between access to EVT and living in more deprived areas is mediated by the distance to EVT-capable centres. This problem is not easy for Canadian policy-makers — who are tasked with providing quality health care to a geographically dispersed population — to solve. However, our findings suggest that improving access to EVT for people in more remote locations would have the additional benefit of ensuring more equitable access to this treatment for those living in more deprived areas. Other investigators have sought to expand the treatment window for EVT based on certain imaging characteristics,9,10 which may improve equity in access to this treatment.
Health care practitioners in remote areas may seek avenues of expediting transfer of potential EVT recipients. Remote robotic EVT is an evolving technology that may offer a means of treating patients from rural areas with EVT before transport, thereby mitigating the effect of distance to a CSC on the likelihood of receiving EVT.34
Future work should attempt to replicate our findings without limiting the study cohort to people treated with alteplase. Furthermore, researchers should investigate whether people from areas with low socioeconomic status experience worse outcomes and have longer times to treatment than those from areas with high socioeconomic status. We did not assess the cost-effectiveness of changes that might result in more equitable distribution of EVT based on neighbourhood socioeconomic deprivation and the distance people live from the nearest CSC. As such, future researchers may wish to perform a distributional cost-effectiveness analysis that accounts for improved equity and the finite resources of Alberta’s health care system.
Limitations
Our cohort was restricted to patients who received alteplase as treatment for their ischemic stroke, which excluded any person who presented outside the window for intravenous thrombolysis. This may have systematically excluded people of low socioeconomic status if they were more likely to present outside the treatment window for alteplase. However, this allowed us to compare for whether any pre-existing disparities in access to acute stroke care were widened by the advent of EVT. Second, our independent variable of interest was neighbourhood-level socioeconomic status, which may not be reflective of a person’s socioeconomic status. Although neighbourhood socioeconomic status is associated with health outcomes, it raises the possibility of the ecological fallacy.35,36 Furthermore, we included distance from a patient’s postal code to the nearest CSC in our logistic regression model. Given that not all strokes occur at home, this may have introduced a source of error into our analysis. Nonetheless, we felt that these were appropriate decisions given the limitations of administrative data, as no more detailed data were readily available. Last, our data set did not contain a variable for ethnicity, which may play a confounding role in the relation between neighbourhood socioeconomic status and treatment decisions.37 However, previous work using the Pampalon index has shown the index to be predictive of adverse health outcomes even after race is accounted for.38
Conclusion
We found a significant difference in the odds of receiving EVT in Alberta after intravenous alteplase treatment for an ischemic stroke based on neighbourhood socioeconomic status. Patients in neighbourhoods with the lowest socioeconomic status tended to live farther from the nearest CSC than patients from less deprived neighbourhoods. Our results suggest that a key avenue for improving the equitable distribution of EVT is to improve access for people who live outside large urban centres. Health care organizations may look to expand access to EVT where adequate numbers of procedures can be assured to maintain quality. Although this would require some resource mobilization, it would increase the equality of access to this disability-saving and, in some cases, life-saving procedure.
Acknowledgements
The authors extend sincere thanks to Paul R. Pival and Renna Truong at the University of Calgary libraries for their assistance in cleaning and organizing the geographic data.
Footnotes
Competing interests: Michael Hill reports grants from Boehringer-Ingelheim to the University of Calgary for the TEMPO-2 and ACT-GLOBAL trials; from Biogen to the University of Calgary; from NoNO to the University of Calgary for the ESCAPE-NA1 and ESCAPE-NEXT trials; from the Canadian Institutes of Health Research to the University of Calgary for the ESCAPE-NA1 and ESCAPE-NEXT trials; from Medtronic to the University of Calgary for the HERMES collaboration; and from Alberta Innovates to the University of Calgary for the QuICR Alberta Stroke Program (some of the funds were used for the ESCAPENA1 trial). He has received consulting fees from Sun Pharmaceutical Industries and BrainsGate for adjudication of clinical trial outcomes. He reports US Patents 62/086,077 and 10,916,346, both licensed to Circle Neurovascular Imaging. He has been chair of the Data and Safety Monitoring Committee for the RACECAT trial (end 2020), the Oncovir Hiltonol trial (end 2023) and the DUMAS trial (end 2023). He is a member of the Data and Safety Monitoring Board for the ARTESIA trial (end 2023) and the BRAIN-AF trial (ongoing). He is president of the Canadian Neurological Sciences Federation and a member of the board of directors of the Canadian Stroke Consortium. He holds private stock in Circle Cardiovascular Imaging and PureWeb. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Matthew Eagles, Reed Beall and Eldon Spackman conceived the study and drafted the manuscript, with contributions from Michael Hill and John Wong. Matthew Eagles, Reed Beall and Eldon Spackman designed the study. Matthew Eagles, Reed Beall and Eldon Spackman acquired the data, with contributions from David Ben-Israel. Matthew Eagles, Reed Beall and Eldon Spackman analyzed the data, with contributions from David Ben-Israel, Michael Hill and John Wong. All authors interpreted the data, revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: Matthew Eagles received funding through the Canadian Institutes of Health Research Canada Graduate Scholarship — Master’s Award.
Data sharing: These data were obtained through the Alberta Stroke Program’s Quality Improvement in Clinical Research Database and Alberta Health Services. They are not freely available. Any interested person should contact these sources for data availability.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/6/E1181/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.